Right-Sided Pneumothorax Associated with Pneumoperitoneum Subsequent to Transverse Colon Perforation: Case Report
A B S T R A C T
Pneumothorax can be spontaneous or secondary to a pre-existing disorder or trauma. Pneumothorax associated with pneumoperitoneum without thoraco-abdominal communication is a rare event poorly described in the literature. We report the case of a 73-year-old patient undergoing abdominal debulking surgery for advanced stage ovarian cancer complicated by a pneumoperitoneum and a right-sided pneumothorax without hernia or evidence of diaphragmatic trauma. Several physio-pathological hypotheses have been suggested, including a potential COVID-19 infection without clear etiology. Our case report emphasizes the possible association of pneumothorax with pneumoperitoneum related to a colon perforation without visible diaphragmatic or mediastinal defects.
Keywords
Pneumothorax, pneumoperitoneum, colon perforation, COVID-19
Introduction
Pneumothorax is a disorder with various etiologies of isolated occurrence in 75% of cases. Primary or idiopathic spontaneous pneumothorax mainly affects young (about 35-year-old), tall, and thin men. The risk of pneumothorax is especially high in people with lung disease and in smokers [1]. Secondary pneumothorax is related to chronic obstructive pulmonary disease (COPD), emphysema, asthma, cystic fibrosis, and endometriosis [2].
Pneumothorax associated with pneumoperitoneum is a rare event [3, 4]. The link between the presence of intrapleural and intraperitoneal air without mediastinal communication has not been demonstrated to date without iatrogenic cause [3, 4]. It is usually related to malformation or diaphragmatic trauma [1, 2]. Pneumoperitoneum suggests the perforation of a hollow organ (stomach, vagina, digestive tract, uterus) [5]. The association of unilateral pneumothorax with pneumoperitoneum subsequent to a colon perforation without pneumo-mediastinum, iatrogenic esophagus, or diaphragmatic injury has not been described to date [3, 6]. We report the case of a patient presenting an extensive right-sided anterior pneumothorax associated with pneumoperitoneum after digestive perforation following ovarian cancer interval surgery.
Case Report
A 73-year-old woman, menopausal since the age of 49 years without hormonal replacement therapy, with a history of five pregnancies (three vaginal deliveries and two miscarriages), was referred to Tenon University Hospital for suspicion of ovarian cancer [7, 8]. The patient had a history of partial thyroidectomy for an unsubstituted benign lesion, mitral valve disease, and a family history of bowel cancer (sibling). She was also severely obese (BMI 36.1 kg/m2), and suffered from hypertension, type-2 diabetes, sleep apnea apparatus syndrome, and COPD obstructive lung disease, which was treated with a long-acting anticholinergic agent. Chest CT scans were normal in 2017 and 2018. The patient was allergic to penicillin.
The patient had consulted in Portugal in December 2019 for acute sciatica. An MRI of the lumbar spine was performed, detecting a pelvic mass with solid and cystic components. On January 10, 2020, the patient consulted in the Gynaecology Unit at Tenon Hospital (France) when the presence of a pelvic mass was confirmed. A second pelvic MRI was performed, showing a 13 cm left adnexal mass with a large solido-cystic tumor (O-RADS 5) attributed to a primary cystadenocarcinoma ovarian cancer with ascites but without carcinosis or pathological pelvic or paraaortic lymph nodes (Figure 1).
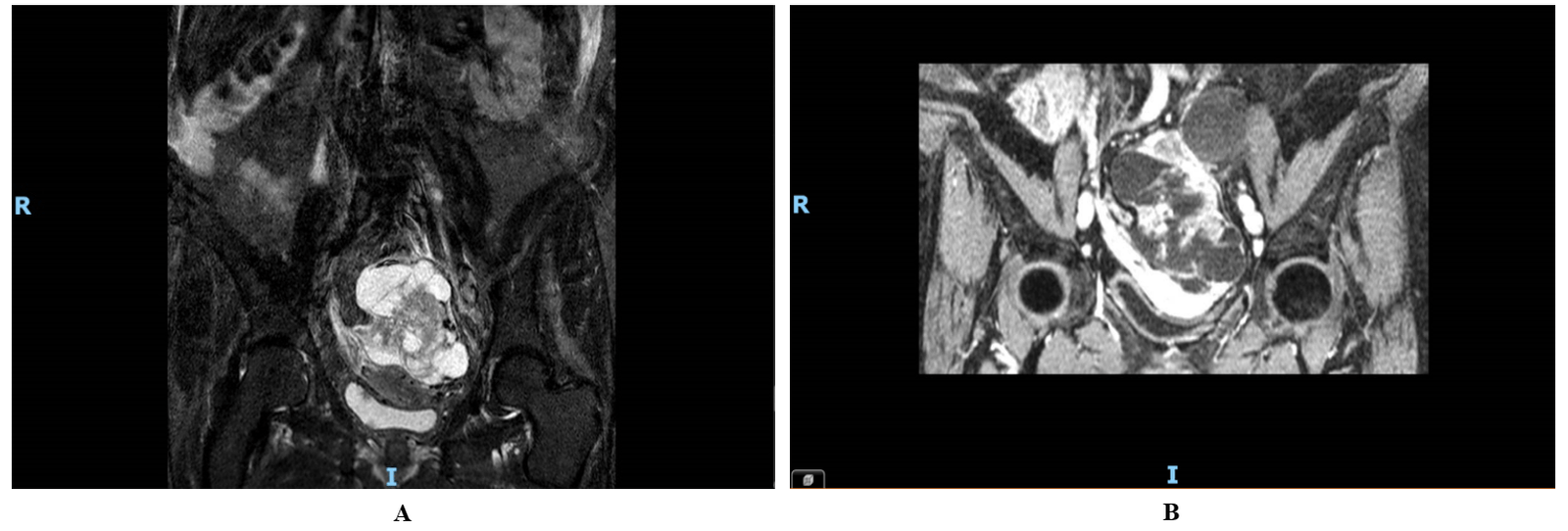
Figure 1: Initial MRI showing a 13 cm left adnexal mass with a large solido-cystic tumor (O-RADS 5) attributed to a primary ovarian cancer with ascites without carcinosis.
A budding polypoid thickening of the posterior bladder wall was detected. A thoraco-abdomino-pelvic (TAP) scan performed on January 17, 2020 confirmed a heterogeneous tissue mass of 140 mm on the left ovary with ascites and peritoneal carcinosis but without suspicious lymph nodes or pyelocaliceal dilation. The thorax scan was normal, but a cervical thyroid nodule was detected (Figure 2). The CA 125 serum level was elevated at 294 U/mL with normal CA 19.9 at 6.2 U/mL.
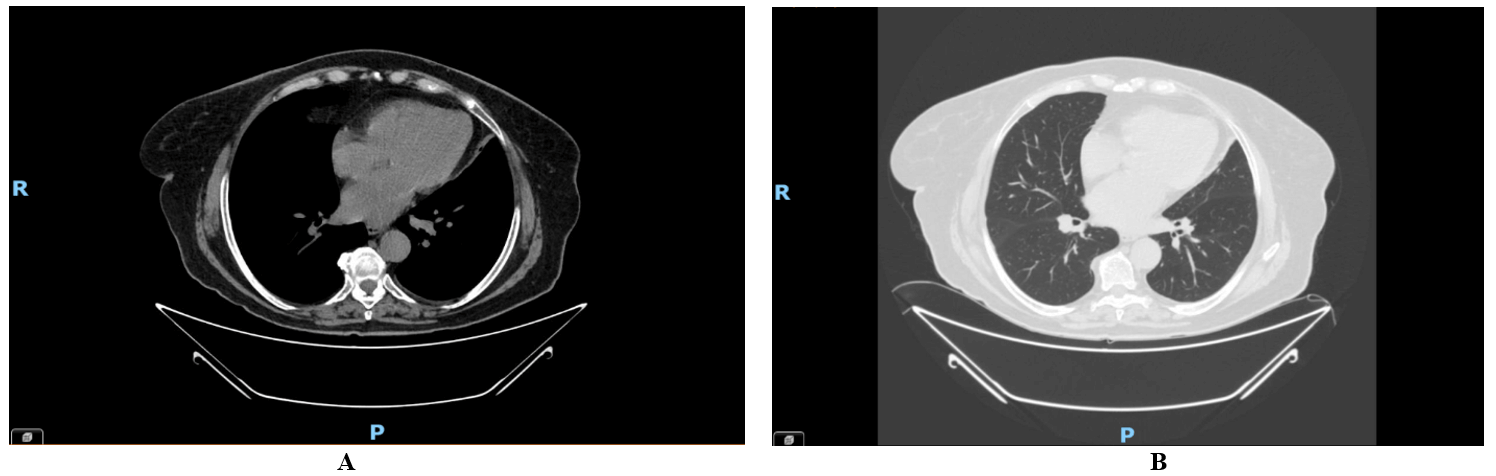
Figure 2: Initial thoraco-abdomino-pelvic (TAP) scan performed on January 17, 2020 showing the absence of pulmonary lesions and pleural effusion.
On January 24, 2020, the patient was referred to a gynaecologic oncology surgeon for suspicion of stage IIIC ovarian cancer. A cervical pap smear and endometrial biopsy were performed, showing no abnormality. A PET-FDG scan was also performed, detecting a large heterogeneous pelvic mass of a highly hypermetabolic neoplastic appearance (SUV max 31.4), a peritoneal carcinosis without suspicious lymph nodes, but a left pleural effusion of low non-hypermetabolic abundance, suggesting stage IVa ovarian cancer. Mammography was classified as BIRADS 2. A cystoscopy was performed confirming a polypoid thickening of the posterior bladder wall suggesting bladder cancer. No additional investigation was performed to explore the thyroid. Diagnostic laparoscopy and operative cystoscopy were performed after a multidisciplinary committee consultation. Laparoscopy revealed a pelvic mass on the left ovary with peritoneal carcinosis involving the omentum and the pelvis. The Sugarbaker score was 5/27, but four abdominal areas were not evaluable. The Fagotti score was 4 and the Makar score was 5 due to neoadjuvant chemotherapy after onco-geriatric consultation.
Omental biopsy revealed a high-grade serous ovarian adenocarcinoma of ovarian origin without somatic BRCA mutation. The peritoneal cytology was positive for tumor cells. A diagnosis of low-grade pTa classified as non-invasive papillary urothelial carcinoma was retained after cystoscopic bladder resection. A double JJ stent was inserted during the cystoscopy because of mucosal resection near the left ureteral meatus. The CA125 serum level was re-evaluated at 570 U/mL. After a second multidisciplinary committee consultation and onco-geriatric evaluation, the patient was administered neoadjuvant chemotherapy consisting of a standard protocol with Paclitaxel-Carboplatin (paclitaxel 175 mg/m2, carboplatin AUC 4 (instead of AUC5, i.e., dose reduction of 20%).
After three cycles of chemotherapy, a CT TAP scan found regression of pleural and intra-peritoneal effusion with persistence of the left pelvic mass. The CA 125 serum level was 17 UI/mL. A second laparoscopy was initially planned for April 20, 2020 but postponed due to the COVID-19 pandemic in accordance with the French recommendations (Francogyn, Collège National des Gynécologues et Obstétriciens Français (CNGOF)) and the patient was administered a fourth chemotherapy cycle. Laparoscopy was finally performed on May 14, 2020, showing no residual carcinomatosis but the persistence of a left ovary tumor. According to the COVID-19 recommendations, a preoperative chest scan was performed the day before the debulking surgery to rule out a COVID-19 infection and showed no suspicious lesions. The COVID-19 PCR was also negative.
Debulking surgery was performed on May 29, 2020, with an initial PCI score rated at 2/39, including a total hysterectomy with bilateral salpingo-oophorectomy, infragastric omentectomy, appendectomy but without pelvic and paraaortic lymphadenectomy because of initial stage IVa and the absence of suspicious lymph nodes intraoperatively. No peritoneal diaphragmatic location was observed. The left JJ stent was removed at the last surgical step after cystoscopic control of the left ureteral meatus. The surgery was considered complete (R0). Histology confirmed the persistence of an active tumor on the left ovary exclusively.
On postoperative day 8, the patient experienced fever with a urinary infection, which was treated with antibiotics (Azactam®, Sanofi-Aventis laboratory, France). A second JJ stent was inserted as a CT urogram revealed hypotonia of the left pyelocaliceal cavities without nephritis. The TAP scan was normal. On day 11, the patient’s temperature was 38°C and she complained of abdominal pain. An additional TAP scan revealed an extensive pneumoperitoneum, mainly in the perigastric area associated with fat infiltration suggesting a gastric perforation, and a right-sided anterior pneumothorax without extension to the mediastinum (Figure 3). No hiatus hernia was detected.

Figure 3: TAP scan on day 11 showing a pneumothorax without pneumomediastinum but associated with pneumoperitoneum.
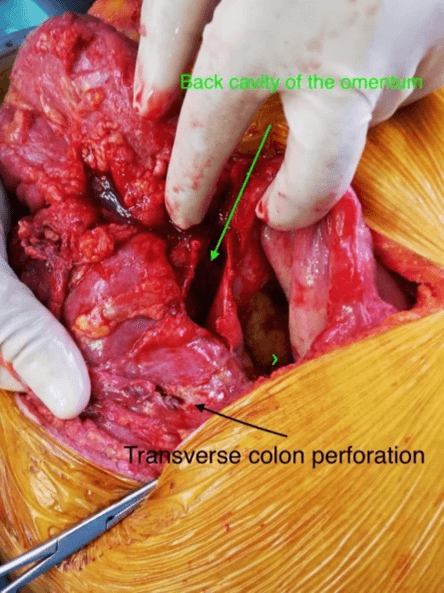
Figure 4: Laparotomic view showing a transverse colon perforation.
A chest drain was placed before a second surgery, which revealed a 1 cm transverse colon perforation with stercoral peritonitis in the retrogastric area, probably subsequent to thermic injury during the omentectomy. A transverse perforation was confirmed at laparotomy after extensive bowel adhesiolysis, and a colostomy was performed on the perforation site (Figure 4). Careful exploration of the right diaphragmatic dome showed no injury, and no air leakage was observed after a pulmonary pressure leak test. Intraoperative bacteriological samples revealed Escherichia coli, Staphylococcus epidermidis, and Enterococcus faecium infection. The total hospital stay was 3 weeks. Adjuvant chemotherapy was completed by three additional cycles with paclitaxel (10% dose reduction) and carboplatin AUC 4 followed by bevacizumab therapy. After 6 months’ follow-up, no recurrence was detected, and the defunctioning stoma was removed.
Discussion
Here we report the case of a right-sided pneumothorax associated with pneumoperitoneum in the context of peritonitis but without diaphragmatic hernia or operative injury. To date, few case reports have been published describing the association of pneumothorax with pneumoperitoneum. Sadik et al. described a case of a 59-year-old patient with diverticular sigmoid perforation but in the context of a known hiatal hernia [5]. Glauser & Bartlett reported five cases of pneumothorax associated with pneumomediastinum: the first case occurred in a 16-year-old boy after intra-abdominal diffusion subsequent to an alveolar rupture due to excessive ventilation pressures; the second occurred in a 39-year-old woman with pneumoperitoneum secondary to high ventilator inspiration pressures (>55 cm Hg) with a potential primary trauma during tracheostomy; the third occurred in a 42-year-old woman with pulmonary insufficiency related to a low cardiac output following an overdose and possible aspiration requiring relatively high ventilatory inspired pressures (45 cm H2O) and the use of PEEP; the fourth occurred in a 40-year-old woman with pneumothorax after a rib trauma potentially explained by high pressures applied to the thoracic cage with air diffusion through a diaphragmatic defect into the abdomen and the retroperitoneal space; and finally, the fifth case occurred in a 50-year-old man exhibiting a pneumothorax subsequent to pneumoperitoneum but without diaphragmatic defect visualized at laparoscopy [3]. This last case seems similar to ours in that no link between pneumoperitoneum and pneumothorax was identified. However, our patient presented some risk factors for pneumothorax, including sleep apnea apparatus syndrome and COPD treated with a long-acting anticholinergic agent. Duarte et al. reported a case of pneumoperitoneum without digestive perforation related to a massive bilateral pneumothorax explained by diaphragmatic defect [4].
In the current case report, several hypotheses could explain the association of pneumothorax with pneumoperitoneum. First, pneumoperitoneum was subsequent to a right-sided pneumothorax via a defect of the right diaphragmatic muscle [3]. As previously mentioned, no diaphragmatic injury or air leakage was observed during the surgery, but the perforation might have been clogged. A few case reports have underlined the relation between pneumothorax and pneumoperitoneum caused by mechanical ventilation, which was not needed in our patient [9-11]. Second, peritonitis with pneumoperitoneum led to pneumothorax by decompensation of COPD or pre-existing emphysema, but no emphysema or lung injury was detected on the preoperative chest scan in our patient [6]. Third, barotrauma related to the first intubation or central line trauma could also be a cause, but this is often associated with pneumo-mediastinum [9]. Fourth, pneumothorax may be linked to COVID-19 disease, although the PCR was negative [12-14]. Several case reports and literature reviews have shown a link between COVID-19 pneumopathy and pneumothorax and pneumomediastinum [12-14].
The mechanism for pneumothorax could involve the explosion of the alveoli during the disease, but pneumomediastinum is rather related to an underlying pathology, notably pre-existing emphysema [12-14]. One article has described a non-surgical pneumoperitoneum related to mechanical ventilation during COVID-19 pneumopathy but without associated pneumothorax or pneumomediastinum [15]. In the current case report, the patient did not display any symptoms of COVID-19, and no suggestive frosted glass lesions were noted on the chest scan. However, COVID-19 infection cannot be definitely ruled out as no additional PCR was done [16].
Conclusion
The association of a pneumothorax subsequent to a colon perforation with pneumoperitoneum can exist even in the absence of a visible diaphragmatic or mediastinum defect. Further case reports are required to clarify the exact physiopathology.
Conflicts of Interest
None.
Article Info
Article Type
Case ReportPublication history
Received: Thu 10, Dec 2020Accepted: Mon 18, Jan 2021
Published: Tue 02, Feb 2021
Copyright
© 2023 Jeremie Benichou. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.JSO.2021.01.02
Figures & Tables
References
- Gupta D, Hansell A, Nichols T, Duong T, Ayres JG (2000) Epidemiology of pneumothorax in England. Thorax 55: 666‑671. [Crossref]
- Rabbat A, Hazouard E, Magro P, Lemarie E (2004) Evidence based pneumology: 3rd update workshop to the SPLF. Management of spontaneous and primary pneumothorax. Rev Mal Respir 21: 1187‑1190. [Crossref]
- Glauser FL, Bartlett RH (1974) Pneumoperitoneum in Association with Pneumothorax. Chest 66: 536‑540. [Crossref]
- Duarte F, Wentling J, Anjum H, Varon J, Surani S (2016) Pneumothorax Causing Pneumoperitoneum: Role of Surgical Intervention. Case Rep Crit Care 2016: 4146080. [Crossref]
- Sadik KW, Vorenberg A, Schirmer B (2009) A Case of Concomitant Pneumothorax and Pneumoperitoneum. J Laparoendosc Adv Surg Tech A 19: 517‑518. [Crossref]
- Noppen M (2010) Spontaneous pneumothorax: epidemiology, pathophysiology and cause. Eur Respir Rev 19: 217‑219. [Crossref]
- ©Conduites à tenir initiales devant des patientes atteintes d’un cancer épithélial de l’ovaire/Synthèse 2018.
- National Comprehensive Cancer Network Inc (2019) NCCN Clinical Practice Guidelines in Oncology: Ovarian Cancer, Version 1.2019. Nat Comprehen Cancer Netw Inc.
- Hsu CW, Sun SF (2014) Iatrogenic pneumothorax related to mechanical ventilation. World J Crit Care Med 3: 8‑14. [Crossref]
- Okamoto A, Nakao A, Matsuda K, Yamada T, Osako T et al. (2014) Non-surgical pneumoperitoneum associated with mechanical ventilation. Acute Med Surg 1: 254‑255. [Crossref]
- Henry RE, Ali N, Banks T, Dais KA, Gooray DA (1986) Pneumoperitoneum associated with mechanical ventilation. J Natl Med Assoc 78: 539‑541. [Crossref]
- Quincho Lopez A, Quincho Lopez DL, Hurtado Medina FD (2020) Case Report: Pneumothorax and Pneumomediastinum as Uncommon Complications of COVID-19 Pneumonia-Literature Review. Am J Trop Med Hyg 103: 1170-1176. [Crossref]
- Ferreira JG, Rapparini C, Gomes BM, Pinto LAC, Freire MS da SE (2020) Pneumothorax as a late complication of COVID-19. Rev Inst Med Trop Sao Paulo 62: e61. [Crossref]
- Poggiali E, Vercelli A, Iannicelli T, Tinelli V, Celoni L et al. (2020) COVID-19, Chronic Obstructive Pulmonary Disease and Pneumothorax: A Frightening Triad. Eur J Case Rep Intern Med 7: 001742. [Crossref]
- Gemio Del Rey IA, de la Plaza Llamas R, Ramia JM, Medina Velasco AA et al. (2020) Non-surgical Spontaneous Pneumoperitoneum in a COVID-19 Positive Patient With Severe Bilateral Pneumonia. Cir Esp. [Crossref]
- Herpe G, Lederlin M, Naudin M, Ohana M, Chaumoitre K et al. (2020) Efficacy of Chest CT for COVID-19 Pneumonia in France. Radiology 202568. [Crossref]