Journals
Right Hepatectomy In Patient with Absent Portal Vein Bifurcation
A B S T R A C T
Introduction: Understanding of hepatic vascular anatomy and its variations are crucial for performing liver resection and transplantation. Here we present a case of successful right hepatectomy in the patient with absent portal vein bifurcation.
Case presentation: 34 years old female presented for elective right hepatectomy. Preoperative CT scan demonstrated absence of portal vein bifurcation. Right hepatectomy was safely achieved by parenchymal division under ultrasound guidance with preservation of intrahepatic portal branches to left hemiliver and without postoperative complications.
Discussion: Normal portal vein anatomy is observed in 65-86% of all cases [1, 2]. Of all portal vein anatomy variations, absence of the portal vein bifurcation is rarest among reported with incidence as low as 0.03% [1].
Conclusion: Preoperative recognition of aberrant portal vein anatomy is important for prevention of life-threatening complications after elective hepatectomy and transplantation.
Keywords
Hepatectomy, portal vein
Introduction
Normal portal vein anatomy is observed in 65-86% of all cases [1, 2]. We present a case of preoperative recognition of rare portal vein anatomy and subsequent uncomplicated right hepatectomy in patient with absent portal vein bifurcation.
Case Report
34 years old female with history of oral contraceptive use and large uterine fibroid presented with 12 cm biopsy proven hepatic adenoma. She was scheduled for elective right hepatectomy. On preoperative CT scan a rare variant of portal anatomy-absence of portal vein bifurcation was noted (Figures 1-2). Patient had single right portal vein entering the liver with intrahepatic branching to left portal vein. During surgery, origin of intrahepatic left portal vein branch was mapped under ultrasound control and preserved during resection. Patient had uncomplicated postoperative course and was discharged on postoperative day 5 without evidence of liver remnant ischemia.
Discussion
Normal portal vein anatomy is observed in 65-86% of all cases [1, 2]. In this scenario, main portal vein bifurcates extrahepatically into right main and left main veins which are then subsequently divided into right anterior (inflow to segments V and VIII) and right posterior (inflow to segments VI and VII) as well as left portal branches to segment IV, segment II and III and caudate lobe3. Portal vein trifurcation (division of main portal vein into right anterior, right posterior and left main portal veins instead of bifurcation) is most common variation with incidence of about 10%. Of all portal vein anatomy variations, absence of the portal vein bifurcation is rarest among reported with incidence as low as 0.03% [1]. In this variation, first described by Couinaud in 1957, single right portal vein enters the liver hilum with variable intrahepatic portal vein branches supplying left hemiliver [2]. If not recognized, severe complications in form of postoperative remnant liver ischemia, portal vein thrombosis and death can be expected [1, 3]. With careful preoperative imaging and planning, successful hepatectomy and liver transplantation can be carried out without difficulty [4, 5].
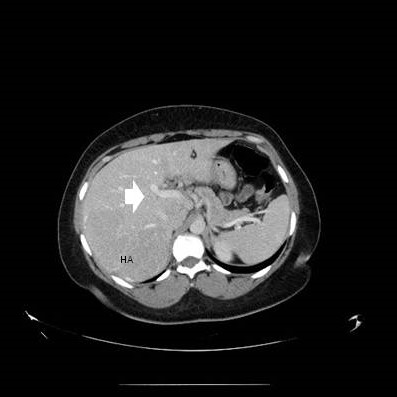
Figure 1: HA indicates hepatic adenoma, white arrow indicates single right portal vein entering the liver
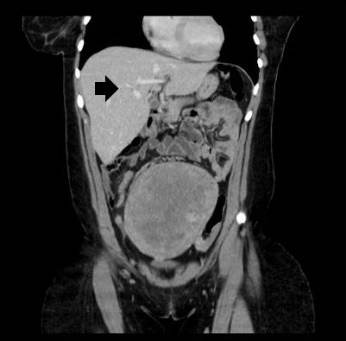

Figure 2 and 3: Black arrow indicates intrahepatic origin of the left portal vein of right portal vein branch.
Conclusion
Preoperative recognition of aberrant portal vein anatomy is important for prevention of life-threatening complications after elective hepatectomy and transplantation.
Conflicts of Interest
The authors declare no conflict of interest.
Funding
No specific funding was used in preparation of this article.
Ethical approval
Exception from ethical approval-case report only, consent from the patient provided at request.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Authors contribution
Conception of the article- MF, CK, AC
Article draft and data gathering- MF, CK, AC
Final review and approval- CK, AC
Registration of research studies
Not required
Guarantor
Andrei Cocieru, MD
Article Info
Article Type
Case ReportPublication history
Received: Fri 14, Jun 2019Accepted: Wed 26, Jun 2019
Published: Sat 06, Jul 2019
Copyright
© 2023 Andrei Cocieru. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.IJSCR.2019.02.01
Author Info
Corresponding Author
Andrei CocieruNortheastern Ohio Medical University, Rootstown, Ohio
Figures & Tables
References
- Chaib E (2009) Absence of bifurcation of the portal vein. Surg Radiol Anat. 31: 389-392. [Crossref]
- Covey AM, Brody LA, Getrajdman GI, Sofocleous CT, Brown KT et al. (2004) Incidence, patterns, and clinical relevance of variant portal vein anatomy. AJR Am J Roentgenol 183: 1055-1064. [Crossref]
- Koh MK, Ahmad H, Watanapa P, Jalleh RP, Habib NA (1994) Beware the anomalous portal vein. HPB Surg 7: 237-239. [Crossref]
- Iqbal S, Iqbal R, Iqbal F (2017) Surgical Implications of Portal Vein Variations and Liver Segmentations: A Recent Update. J Clin Diagn Res 11: AE01-AE05. [Crossref]
- Yamamoto H, Nagino M, Kawabata Y, Maki A, Takenouchi Y et al. (2000) Resection of a hilar cholangiocarcinoma in a patient with absent portal bifurcation. Hepatogastroenterology 47: 362-364. [Crossref]
- Mitchell A, Mirza D, de Ville de Goyet J, Buckels J (2000) Absence of the left portal vein: a difficulty for reduction of liver grafts? Transplantation 69: 1731-1732. [Crossref]