Relationship Between Styloid Process Size and the Skeletal Craniofacial Pattern: A Cross-Sectional Study
A B S T R A C T
Objective: The purpose of this correlation study was to evaluate a possible association between the styloid process size and different craniofacial skeletal patterns, in the sagittal and the vertical planes.
Methods: 59 consecutive orthodontic adult patients were selected. The styloid process length was measured on pretreatment panoramic radiographs and the cephalometric skeletal variables on lateral cephalometric radiographs. Data were analyzed using independent sample T-Tests, Mann-Whitney U Tests and Spearman´s partial correlations (=5%).
Results: Males exhibited longer styloid processes than females (p=0.029), with a mean difference of 7.5mm. Within each individual, right and left styloid process length was similar (r= 0.77; p<0.001). No relationship was found between the size of the styloid process and the sagittal skeletal pattern. A moderate significant correlation was present between the size of the styloid process and some vertical cephalometric skeletal variables: Ar-Go-Me (r=0.32; p=0.02), PFH/AFH (r=-0.29; p=0.03) and MP-SN (r=0.28; p=0.03).
Conclusion: Longer styloid processes tend to be associated with high angle skeletal patterns. Orthodontists, general dentists and oral surgeons should be aware that elongation of the styloid process is more frequently verified in hyperdivergent individuals.
Keywords
Styloid process length, Cephalometric variables, Vertical pattern, Sagittal pattern
Introduction
The first case of stylohyoid ligament ossification was reported in 1652, by Demanchetis. Although Weinleche later described the clinical signs and the surgical procedures to remove the styloid process, this entity was only named after Dr. Watt Eagle, which fully described its symptoms, diagnosis, and treatment. The Eagle syndrome (ES) implies stylalgia, and is characterized as an elongated or malpositioned styloid process, occuring with pain [1-3]. The styloid process is a conical osseous outgrowth on the inferior surface of the temporal bone, that develops embryologically as part of the stylohyoid complex [4]. This consists of the styloid process, the stylohyoid ligament and the lesser cornu of the hyoid bone [5].
All structures of the stylohyoid complex are derived from the Reichert's cartilage, which arises during embryogenesis from the second pharyngeal arch [6]. Although typically straight, it can occasionally be curved [6]. Styloid process insertions include the stylopharyngeus, styloglossus and stylohyoid muscles, and the stylomandibular and stylohyoid ligaments [4]. The normal styloid process measures approximately 2.5 to 3 cm, above which it is considered elongated [1, 2]. This condition may be uni or bilateral [1, 2]. Variations could be observed in the process length, thickness, angle and direction of the deviation, ossification degree and position of the process on the surface of the temporal bone. Several imagiological classifications have been proposed to standardize the description of these different structures [5, 7]. Mineralization of the stylohyoid process or stylohyoid-stylomandibular ligament complex is a quite common anatomical finding [8].
Its prevalence is highly variable, due to true differences in the populations, or differences in the measurements criteria [6, 8-13]. Studies based on analysis of panoramic radiographs in various populations have shown a prevalence of 1% to 84.4% [6, 8-13]. Elongation of the styloid process can be relevant, when is accompanied with symptoms [8]. Although no consensus in the literature was found regarding the frequency of the styloid process elongation, only a small number of elongated cases present symptoms (4%) [14]. Eagle´s syndrome may be associated to a wide range of clinical manifestations, differing on the main pathogenic process [6]. Eagle distinguished two types, the typical syndrome and the carotid artery syndrome [2]. The first type can present ear pain, neck pain extending to the oral cavity and the maxilla, dysphagia, persistent sore throat, dysphonia, odynophagia, trismus, vertigo and tinnitus, tongue pain, a feeling of hypersialia, vocal changes, taste changes, and pain in the upper limbs, chest, and the temporomandibular joint [6].
In the carotid artery syndrome type, pain along the artery, eye, sight disturbances, facial and parietal cephalgia, aphasia, weakness or even syncope episodes can be present [6]. The differential diagnosis includes a wide range of diseases on the cranial, cervicofacial and cervicopharyngeal regions. Stylalgia can be confused with dental caries, impacted third molars, temporomandibular joint disorders, neuralgias, tongue tumors or even submandibular sialolithiasis [15, 16]. Different theories have been suggested on the etiology of the elongated styloid process: genetic, as an autosomal recessive or dominant trait; acquired, as an anatomical variation, an hyperplasia or a metaplasia resulting from trauma; abnormal development for age, where the loss of elasticity of soft cervical tissues results in increased resistance to joint movement; proliferation of mineralized tissue in the stylohyoid ligament insertion zone, resulting from endocrine dysfunction in postmenopausal women; a degenerative process with consequent ossification, in patients with rheumatoid disease; or idiopathic [6, 17-19].
Patients with an elongated styloid process may be directed to the orthodontic clinic, with the complaint of orofacial and craniocervical pain [15]. However, there is a gap in the orthodontic knowledge on this subject, and only one case report has been found in the literature [15]. Due to the muscles and ligaments inserted on the styloid process, its size could be directly related to different craniofacial structures, such as the pharynx, the larynx, the tongue, the hyoid bone and the mandible. Although some cephalometric studies have described the craniofacial pattern variation related to the hyoid bone, no studies have been found for the styloid process [20, 21]. Therefore, the objective of the present research was to evaluate a possible association between the size of styloid process and different craniofacial skeletal patterns, in the sagittal and the vertical dimensions.
Materials and Methods
Data for the present study was collected from the records of the UL School of Dentistry Orthodontics Department, after approval by the UL School of Dentistry Ethics Review Board. A consecutive sample was gathered from records over a period of 11 years, ending in September of 2018. The inclusion criteria were European ancestry, 18 to 22 years of age by the time of the first orthodontic appointment, good quality cephalometric and panoramic x-rays obtained in the same machine (Orthopantomograph OP100 and Orthoceph OP100, General Electric Company, Finland), good general health, no clinical history of facial trauma and no history of orthodontic, orthopedic or surgical treatments. Patients that were not in the sixth stage of the cervical vertebral maturation method (CVM) were excluded [22]. Figure 1 shows the flow diagram of the selection process of the final 59 individuals.
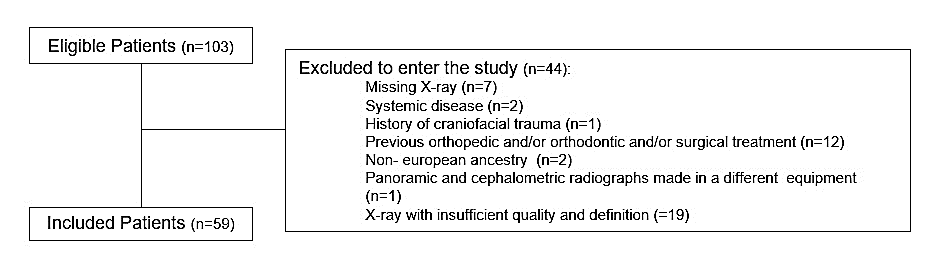
Figure 1: Patient flow chart.
I Radiograph Analysis
The cephalometric radiographs were traced using Quick Ceph 2000 version 3.6 (Quick Ceph Systems, San Diego CA, USA). The brightness and contrast were adjusted as needed, to improve visualization of the interest area. The zoom tool was used magnify and refine the tracing. For each cephalometric radiograph, 11 landmark points and 6 cephalometric angular measurements were determined, which are represented in the (Figures 2 & 3). The calculated ratios were posterior facial height to anterior facial height (PFH/AFH) and lower third facial height to anterior facial height (ANS-Me/AFH). The sagittal pattern was defined by the ANB angle as Class I (0º≤ANB≤4º), Class II (ANB>4º) and Class III (ANB<0º). The vertical pattern was defined by the MP-SN angle as normodivergent (27º≤MP-SN≤37º), hyperdivergent (MP-SN> 37º), and hypodivergent (MP-SN<27º).
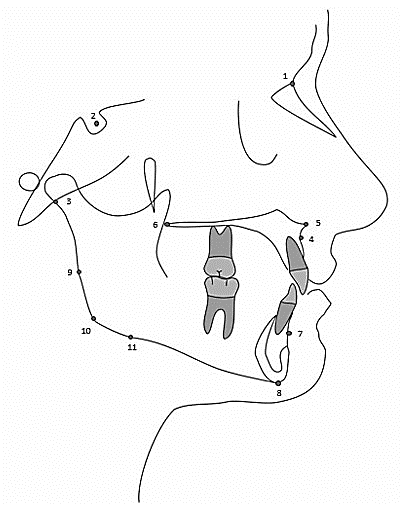
Figure 2: Cephalometric landmark points.
1. Nasion (N): The most anterior midline point on the fronto-nasal suture.
2. Sella (S): The center of the radiographic ouline of Sella Turcica, as determined by inspection.
3. Articulare (Ar): The intersection of the radiographic images of the inferior surface of the cranial base and the posterior surface of the condylar necks of the mandible.
4. Subspinale (Point A): The deepest midline point on the anterior outline of the maxilla between the anterior nasal spine and the alveolar process.
5. Anterior Nasal Spine (ANS): The most anterior midline point on the nasal spine of the maxilla.
6. Posterior Nasal Spine (PNS): The most posterior midline point on the palatal shelves of the palatine bones.
7. Supramentale (Point B): The deepest midline point on the anterior outline of the mandible between the symphysis and the alveolar process.
8. Menton (Me) : The most inferior midline point on the symphysis of the mandible, relative to the Y-axis.
9. Ramus Reference Point (RRef): The most posterior point on the angle of the mandible.
10. Gonion (Go): The most posterior and inferior point on the angle of the mandible.
11. Body Reference Point (BRef): The most inferior point on the angle of the mandible.
All panoramic radiographs were hand-traced on 100m matte acetate paper using a 0.5 mm 4HB pencil on a negatoscope. The styloid process length was measured as described by Andrade et al. (2012). After identifying the contour of the external auditory canal, the length of the styloid process was measured from the lowest point of the external acoustic meatus, to the tip of the process (Figure 4) [23]. The absolute measurements were then divided by the magnification correction factor of 1.23, reported by the manufacturer (Orthopantomograph OP100, General Electric Company, Finland).
II Statistical and Error Analysis
Minimum sample size (n=38) was determined with an exact test for correlation, considering r=0 as the null hypothesis and r≥0,5 as the alternative hypothesis, with alpha set at 0,05 and 95% power (G*Power 3.1.9.2).
To assess the reproducibility of the method, 25 subjects were randomly selected and all the measurements were repeated by the same operator (CS), at least with one month interval [24]. The random error was calculated using the ICC (intraclass correlation coefficient) and the systematic error by the paired Student T-test for all pairs of variables [24, 25]. Wilcoxon's test was performed for the two variables that rejected normality with the Shapiro-Wilk test (length of left styloid process and SNA angle).
The mean, range, and standard deviation values were calculated for the styloid process length and for all the cephalometric variables. The normality of the distribution of the variables was verified by means of the Kolmogorov-Smirnov and the Shapiro-Wilk tests. Independent samples T-Test and Mann-Whitney U Test were used to evaluate differences in age, process length and cephalometric variables, across gender categories. Spearman’s coefficient regarding correlation between styloid process length and cephalometric variables was computed for the full data set, and for the data stratified by gender. The level of significance was set at 0.05, and analysis was performed using software SPSS ® Statistics for Windows, version 24.
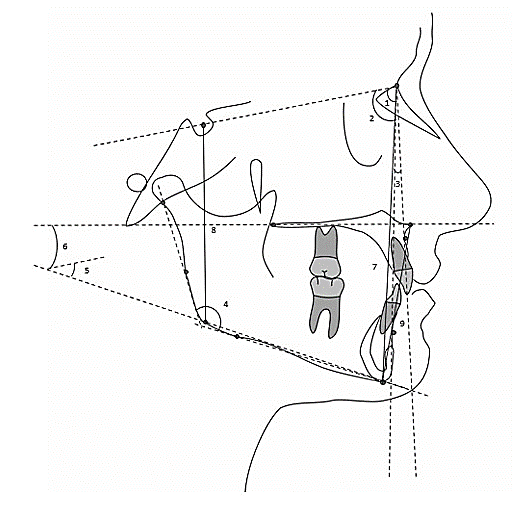
Figure 3: Cephalometric measurements.
1. SNA: The internal angle formed by the intersection of line segments from points Sella to Nasion and from Nasion to Subspinale.
2. SNB: The internal angle formed by the intersection of line segments from points Sella to Nasion and from Nasion to Supramentale.
3. ANB: The acute angle formed by the intersection of line segments from points Subspinale to Nasion and from Nasion to Supramentale. Direction is determined by subtracting SNB from SNA.
4. Gonial Angle: The internal angle formed by the intersection of the ramal line (Ar-RRef) and the mandibular plane (BRef-Me).
5. Mandibular Plane Angle (MP-SN): The acute angle formed by the intersection of line segments S-Na and Go-Me.
6. Palatal Plane- Mandibular Plane (PP-MP): The acute angle formed by the intersection of line segments ANS-PNS and Go-Me.
7. Anterior Facial Height (AFH): The distance measured from Nasion to Menton.
8. Posterior Facial Height (PFH): The distance measured from Sella to Gonion.
9. ANS-Me: The distance measured from Anterior Nasal Spine to Menton.

Figure 4: Linear Measurements on panoramic radiograph.
Results
The intra-class correlation coefficients between the first and second measurements were above 0.90 on all variables, except for the gonial angle (ICC=0.74). This indicates great and moderate reliability, respectively. Student T-test and Wilcoxon's test also did not show significant differences between the two repeated measurements. The descriptive statistics are presented in (Table 1). The mean age (±SD) of the sample was 20.0 (±1.5) years. The mean length of the styloid process was 29.3 mm (±12.2). The cephalometric mean values revealed a Class I relationship with an ANB angle of 3.0 (±2.6) degrees, and a mean normodivergent relationship, with a MP-SN angle of 34.2 (±6.2) degrees.
Table 1: Descriptive statistics referring to continuous variables under study.
|
Variable |
x̅ (sd) |
[min, max] |
|
Age, years |
20.0 (1.5) |
[18.0, 22.0] |
|
Length of styloid process, mm |
29.3 (12.2) |
[3.3, 55.9] |
|
Length of right styloid process, mm |
29.4 (13.2) |
[3.7, 56.9] |
|
Length of left styloid process, mm |
29.1 (12.5) |
[2.9, 54.9] |
|
SNA, º |
79.9 (3.6) |
[71.8, 90.8] |
|
SNB, º |
76.9 (3.9) |
[66.7, 86.5] |
|
ANB, º |
3.0 (2.6) |
[-5.1, 9.7] |
|
Ar-Go-Me, º |
124.4 (5.5) |
[112.6, 135.0] |
|
PFH/AFH, % |
65.0 (4.9) |
[50.6, 75.5] |
|
ANS-Me/AFH, % |
56.8 (2.4) |
[51.0, 60.4] |
|
MP-SN, º |
34.2 (6.2) |
[22.9, 55.3] |
|
PP-MP, º |
26.5 (5.9) |
[13.9, 45.8] |
x̅: sample mean, sd: sample standard derivation, min: minimum, max: maximum, mm: millimiter,: degree. Length of styloid process was calculated with the mean length of right and left styloid process.
Table 2: Comparison by gender of continuous variables under study.
|
|
Gender |
|
|||
|
Female (n=42) |
Male (n=17) |
|
|||
|
Variable |
x̅ (sd) |
[min, max] |
x̅ (sd) |
[min, max] |
P value |
|
Age, years |
20.1 (1.6) |
[18.0,22.0] |
19.8 (1.3) |
[18.0,22.0] |
0.510b |
|
Length of styloid process, mm |
27.1 (12.3) |
[3.3,48.4] |
34.6 (10.6) |
[5.7,55.9] |
0.029* b |
|
SNA, º |
80.4 (3.4) |
[74.3,90.8] |
78.7 (3.9) |
[71.8,84.2] |
0.112 ª |
|
SNB, º |
77.1 (4.0) |
[66.7,86.5] |
76.2 (3.4) |
[67.6,81.1] |
0.428 ª |
|
ANB, º |
3.2 (2.9) |
[-5.1,9.7] |
2.5 (1.9) |
[-2.7,5.9] |
0.336 b |
|
Ar-Go-Me, º |
1247 (5.3) |
[112.6,135.0] |
123.8 (6.1) |
[113.0,133.9] |
0.605 ª |
|
PFH/AFH, % |
64.2 (5.0) |
[50.6,75.5] |
66.9 (4.1) |
[59.2,74.4] |
0.055 ª |
|
ANS-Me/AFH, % |
56.7 (2.4) |
[51.0,60.2] |
57.1 (2.3) |
[53.6,60.4] |
0.624 ª |
|
MP-SN, º |
34.7 (6.6) |
[22.9,55.3] |
33.1 (5.1) |
[26.3,43.8] |
0.386 ª |
|
PP-MP, º |
26.8 (6.2) |
[13.9,45.8] |
25.8 (5.0) |
[16.7,35.6] |
0.552 ª |
x̅: sample mean, sd: sample standard deviation, min: minimum, max: maximum, mm: millimiter, º: degree, *p<0 .05, **p<0 .01, ***p< 0.001. Length of styloid process was calculated with the mean length of right and left styloid process, a Independent samples T Test, b Mann-Whitney U Test.
Table 3: Spearman's correlation matrix for continuous variables under study, controlling length of styloid process by gender.
|
Correlations |
Length of styloid process |
|
|
|
Spearman's rho, r |
P value |
|
Age |
-0.040 |
0.767 |
|
SNA |
-0.017 |
0.897 |
|
SNB |
-0.063 |
0.637 |
|
ANB |
0.087 |
0.518 |
|
Ar-Go-Me |
0.319 |
0.015* |
|
PFH/AFH |
-0.288 |
0.028* |
|
ANS-Me/AFH |
-0.080 |
0.550 |
|
MP-SN |
0.282 |
0.032* |
|
PP-MP |
0.190 |
0.153 |
r: correlation coefficient, P value: sig. (2-tailed), *p<0 .05, **p<0 .01, ***p< 0.001. Length of styloid process was calculated with the mean length of right and left styloid process.
The Spearman’s correlation tests showed a significant correlation between the length of the right and the left styloid process: rho = 0.77 (p <0.001) for the whole sample, rho = 0.57 (p= 0.02) for males, and rho = 0.80 (p <0.001) for females. When divided by gender, statistically significant differences in the length of the styloid process were observed:34.6 mm (±10.6) in males and 27.1 mm (±12.3) in females (Table 2). When controlled for gender, a moderate correlation was found between the size of the styloid process and three vertical skeletal cephalometric variables: Ar-Go-Me (r=0.32; p=0.02), PFH/AFH (r=-0.29; p=0.03) and MP-SN (r=0.28; p=0.03) (Table 3). The results of descriptive statistics across sagittal and vertical patterns are shown in (Table 4).
Table 4: Descriptive statistics referring to categoric variables under study.
|
|
n |
x̅ (sd) |
[min, max] |
|
|
Sagittal Pattern
|
CL I |
36 |
29.6 (11.8) |
[8.9, 55.9] |
|
CL II |
18 |
29.0 (13.4) |
[3.3, 48.4] |
|
|
CL III |
5 |
27.5 (12.8) |
[5.7, 39.8] |
|
|
|
|
|
|
|
|
Vertical Pattern |
Hypodivergent |
6 |
23.4 (8.2) |
[8.9, 33.7] |
|
Normodivergent |
37 |
28.1 (11.5) |
[3.3, 45.3] |
|
|
Hyperdivergent |
16 |
34.2 (13.9) |
[7.9, 55.9] |
Class I (0º£ANB£4º) class II (ANB>4º) class III (ANB<0º), hypodivergent (MP-SN<27º) normodivergent (27º£MP-SN£37º) hyperdivergent (MP-SN> 37º), x̅: sample mean, sd: sample standard deviation, min: minimum, max: maximum *p<0 .05, **p<0 .01, ***p< 0.001.
Discussion
Elongation of the styloid process has been debated in a few studies in the literature. Since this clinical situation can be associated with pain, it should be considered when a differential diagnosis is made. According to the majority of research, the prevalence of elongation increases in older individuals [10-12]. This phenomenon could be caused by degeneration of the ligamentous complex, and a generalized tendency for deposition of calcium salts, related with age [5]. In the present study a restricted age group was chosen, to ensure that growth had ended, and to minimize the aging bias. European ancestry individuals were chosen to minimize the ethnic bias. The inclusion criteria included good general health, no history of trauma and no history of orthopedic, orthodontic, or orthognathic treatment. Although causes for the condition are still uncertain, some clinical situations such as pharyngeal trauma, endocrine dysfunctions in menopausal women, rheumatoid arthritis, renal chronic disease, or psychiatric disorders, have been associated with styloid process elongation [6].
The panoramic radiograph is a valuable and reliable tool for the styloid process length analysis, not only in qualitative but also in a quantitative way [13, 23]. Additionally, it is considered a routine exam taken in almost every dental practice, as it is easy to collect; it eliminates the styloid process overlapping issue that frequently occurs in cephalograms and it has a much lower radiation dose and lower cost than CT or CBCT, which are considered the gold standard for diagnosis of the elongated styloid process [6, 12, 23]. The demographic data in the present research was similar to those reported in previous articles; women seek orthodontic treatment more frequently than men, and most patients have skeletal class I and a mesofacial pattern [26-28].
The average size of the styloid processes in the present sample of 29.3 mm, fits into the normal range described by Eagle, of 25 to 30 mm [1, 2]. The high standard deviation (±12.2) and the high range (minimum of 3.3 and maximum of 55.9) seem to indicate a great individual variability. A strong statistical correlation (r= 0.767, p<0.001) was found between the length of the right (29.4 mm) and the left (29.1 mm) styloid processes. Our findings were consistent with other studies published [13, 23, 29]. Although there is no consensus regarding the presence of elongated styloid process and the affected side, most patients have unilateral complaints[3, 9-12]. Since the etiology of the elongation is not clear, a reason was not suggested for these results [12].
In the present sample, males exhibited longer styloid processes than females with a mean difference of 7.5mm (p=0.03) (Table 2). This sexual dimorphism is probably due to the higher stature of males in comparison to females [30]. The gender distribution is controversial in the literature: some authors found a higher prevalence of elongation in males, others found it in females and others found no significant differences [8-13, 29]. This variation is suggestive that gender might be an irrelevant aspect in the etiology of styloid process elongation. Previous literature has shown that the concept of normality of the styloid process size is variable. Eagle documented an average length from 25 to 30 mm, but recent reports suggest different cut-off values [1, 2, 13]. In this study the mean styloid process size in males was 34.6 mm, which is relatively long. Records of adult stature since the industrial revolution have shown an unprecedented increase which could explain this finding [30].
The relationship between the size of the styloid process and the skeletal pattern was never searched by other investigators. Hypothetically, larger styloid processes could influence mandibular growth through its muscle and ligament insertions [5, 6]. However, in the present study no relationship was found between the size of the styloid process and the sagittal skeletal pattern. Probably the styloid process length could be more influenced by other anatomic structures, such as the pharynx, larynx, tongue and the hyoid bone. The few publications that relate the length of the styloid process with function, seem to indicate that an elongated styloid process can lead to dysfunction of the stomatognathic system and stylalgia [13].
Regarding the vertical skeletal pattern, a moderate correlation was found between the size of the styloid process and some cephalometric vertical skeletal variables, when controlled by gender. A longer styloid process could lead to a shorter and tenser stylomandibular ligament, with the consequent clockwise rotation of the mandible, opening of the gonial angle and a decrease in the PFH/AFH ratio, as shown in the present study (Table 3). Furthermore, since the styloid process is a predominantly vertical anatomical structure, it seems logical to find a larger size in dolichofacial patterns. It was not possible to clearly define pathognomonic cephalometric characteristics of patients with longer styloid processes. However, this research provides insight into the anatomical basis of longer styloid process, which can be a clinical guideline for general dentists, orthodontists, maxillofacial surgeons and other medical specialties.
In the future, longitudinal studies could give more information regarding the size of the styloid process in different skeletal patterns. The relation between aging and a progressive increase in the number of patients with an elongated styloid process or even a progressive increase of the elongation itself could be investigated. Moreover, the relationship between the styloid process size and function or other anatomic structures like the airway space, the tongue and the hyoid bone, needs further research.
Conclusion
Results support the following conclusions:
i. Males have longer styloid processes than females.
ii. Right and left styloid processes tend to have similar sizes in the same subject.
iii. There was no relationship between the sagittal skeletal pattern and the size of the styloid process
iv. High angle patterns tend to be associated with longer styloid processes.
Funding
None.
Competing Interest
None.
Acknowledgement
None.
Article Info
Article Type
Research ArticlePublication history
Received: Wed 19, Feb 2020Accepted: Mon 09, Mar 2020
Published: Mon 23, Mar 2020
Copyright
© 2023 Carolina Santos. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.DOBCR.2020.01.07
Figures & Tables
Table 1: Descriptive statistics referring to continuous variables under study.
|
Variable |
x̅ (sd) |
[min, max] |
|
Age, years |
20.0 (1.5) |
[18.0, 22.0] |
|
Length of styloid process, mm |
29.3 (12.2) |
[3.3, 55.9] |
|
Length of right styloid process, mm |
29.4 (13.2) |
[3.7, 56.9] |
|
Length of left styloid process, mm |
29.1 (12.5) |
[2.9, 54.9] |
|
SNA, º |
79.9 (3.6) |
[71.8, 90.8] |
|
SNB, º |
76.9 (3.9) |
[66.7, 86.5] |
|
ANB, º |
3.0 (2.6) |
[-5.1, 9.7] |
|
Ar-Go-Me, º |
124.4 (5.5) |
[112.6, 135.0] |
|
PFH/AFH, % |
65.0 (4.9) |
[50.6, 75.5] |
|
ANS-Me/AFH, % |
56.8 (2.4) |
[51.0, 60.4] |
|
MP-SN, º |
34.2 (6.2) |
[22.9, 55.3] |
|
PP-MP, º |
26.5 (5.9) |
[13.9, 45.8] |
x̅: sample mean, sd: sample standard derivation, min: minimum, max: maximum, mm: millimiter,: degree. Length of styloid process was calculated with the mean length of right and left styloid process.
Table 2: Comparison by gender of continuous variables under study.
|
|
Gender |
|
|||
|
Female (n=42) |
Male (n=17) |
|
|||
|
Variable |
x̅ (sd) |
[min, max] |
x̅ (sd) |
[min, max] |
P value |
|
Age, years |
20.1 (1.6) |
[18.0,22.0] |
19.8 (1.3) |
[18.0,22.0] |
0.510b |
|
Length of styloid process, mm |
27.1 (12.3) |
[3.3,48.4] |
34.6 (10.6) |
[5.7,55.9] |
0.029* b |
|
SNA, º |
80.4 (3.4) |
[74.3,90.8] |
78.7 (3.9) |
[71.8,84.2] |
0.112 ª |
|
SNB, º |
77.1 (4.0) |
[66.7,86.5] |
76.2 (3.4) |
[67.6,81.1] |
0.428 ª |
|
ANB, º |
3.2 (2.9) |
[-5.1,9.7] |
2.5 (1.9) |
[-2.7,5.9] |
0.336 b |
|
Ar-Go-Me, º |
1247 (5.3) |
[112.6,135.0] |
123.8 (6.1) |
[113.0,133.9] |
0.605 ª |
|
PFH/AFH, % |
64.2 (5.0) |
[50.6,75.5] |
66.9 (4.1) |
[59.2,74.4] |
0.055 ª |
|
ANS-Me/AFH, % |
56.7 (2.4) |
[51.0,60.2] |
57.1 (2.3) |
[53.6,60.4] |
0.624 ª |
|
MP-SN, º |
34.7 (6.6) |
[22.9,55.3] |
33.1 (5.1) |
[26.3,43.8] |
0.386 ª |
|
PP-MP, º |
26.8 (6.2) |
[13.9,45.8] |
25.8 (5.0) |
[16.7,35.6] |
0.552 ª |
x̅: sample mean, sd: sample standard deviation, min: minimum, max: maximum, mm: millimiter, º: degree, *p<0 .05, **p<0 .01, ***p< 0.001. Length of styloid process was calculated with the mean length of right and left styloid process, a Independent samples T Test, b Mann-Whitney U Test.
Table 3: Spearman's correlation matrix for continuous variables under study, controlling length of styloid process by gender.
|
Correlations |
Length of styloid process |
|
|
|
Spearman's rho, r |
P value |
|
Age |
-0.040 |
0.767 |
|
SNA |
-0.017 |
0.897 |
|
SNB |
-0.063 |
0.637 |
|
ANB |
0.087 |
0.518 |
|
Ar-Go-Me |
0.319 |
0.015* |
|
PFH/AFH |
-0.288 |
0.028* |
|
ANS-Me/AFH |
-0.080 |
0.550 |
|
MP-SN |
0.282 |
0.032* |
|
PP-MP |
0.190 |
0.153 |
r: correlation coefficient, P value: sig. (2-tailed), *p<0 .05, **p<0 .01, ***p< 0.001. Length of styloid process was calculated with the mean length of right and left styloid process.
Table 4: Descriptive statistics referring to categoric variables under study.
|
|
n |
x̅ (sd) |
[min, max] |
|
|
Sagittal Pattern
|
CL I |
36 |
29.6 (11.8) |
[8.9, 55.9] |
|
CL II |
18 |
29.0 (13.4) |
[3.3, 48.4] |
|
|
CL III |
5 |
27.5 (12.8) |
[5.7, 39.8] |
|
|
|
|
|
|
|
|
Vertical Pattern |
Hypodivergent |
6 |
23.4 (8.2) |
[8.9, 33.7] |
|
Normodivergent |
37 |
28.1 (11.5) |
[3.3, 45.3] |
|
|
Hyperdivergent |
16 |
34.2 (13.9) |
[7.9, 55.9] |
Class I (0º£ANB£4º) class II (ANB>4º) class III (ANB<0º), hypodivergent (MP-SN<27º) normodivergent (27º£MP-SN£37º) hyperdivergent (MP-SN> 37º), x̅: sample mean, sd: sample standard deviation, min: minimum, max: maximum *p<0 .05, **p<0 .01, ***p< 0.001.
1. Nasion (N): The most anterior midline point on the fronto-nasal suture.
2. Sella (S): The center of the radiographic ouline of Sella Turcica, as determined by inspection.
3. Articulare (Ar): The intersection of the radiographic images of the inferior surface of the cranial base and the posterior surface of the condylar necks of the mandible.
4. Subspinale (Point A): The deepest midline point on the anterior outline of the maxilla between the anterior nasal spine and the alveolar process.
5. Anterior Nasal Spine (ANS): The most anterior midline point on the nasal spine of the maxilla.
6. Posterior Nasal Spine (PNS): The most posterior midline point on the palatal shelves of the palatine bones.
7. Supramentale (Point B): The deepest midline point on the anterior outline of the mandible between the symphysis and the alveolar process.
8. Menton (Me) : The most inferior midline point on the symphysis of the mandible, relative to the Y-axis.
9. Ramus Reference Point (RRef): The most posterior point on the angle of the mandible.
10. Gonion (Go): The most posterior and inferior point on the angle of the mandible.
11. Body Reference Point (BRef): The most inferior point on the angle of the mandible.
1. SNA: The internal angle formed by the intersection of line segments from points Sella to Nasion and from Nasion to Subspinale.
2. SNB: The internal angle formed by the intersection of line segments from points Sella to Nasion and from Nasion to Supramentale.
3. ANB: The acute angle formed by the intersection of line segments from points Subspinale to Nasion and from Nasion to Supramentale. Direction is determined by subtracting SNB from SNA.
4. Gonial Angle: The internal angle formed by the intersection of the ramal line (Ar-RRef) and the mandibular plane (BRef-Me).
5. Mandibular Plane Angle (MP-SN): The acute angle formed by the intersection of line segments S-Na and Go-Me.
6. Palatal Plane- Mandibular Plane (PP-MP): The acute angle formed by the intersection of line segments ANS-PNS and Go-Me.
7. Anterior Facial Height (AFH): The distance measured from Nasion to Menton.
8. Posterior Facial Height (PFH): The distance measured from Sella to Gonion.
9. ANS-Me: The distance measured from Anterior Nasal Spine to Menton.
References
- Eagle WW (1937) Elongated Styloid Process - Report of Two Cases. Arch Otolaryngol 584-587.
- Eagle WW (1948) Elongated Styloid Process; Further Observations and a New Syndrome. Arch Otolaryngol 47: 630-640. [Crossref]
- Härmä R (1967) Stylalgia: Clinical Experiences of 52 Cases. Acta Oto-Laryngologica 63: 149-155.
- Rouviere H, D A, Anatomia Humana, Descriptiva, Topográfica y Funcional, Tomo 1 Cuello Y Cabeza. 11a ed. 2005, Masson.
- Başekim CÇ, Mutlu H, Güngör A, Şilit E, Pekkafali Z et al. (2005) Evaluation of Styloid Process by Three-Dimensional Computed Tomography. Eur Radiol 15: 134-139. [Crossref]
- Piagkou M, Anagnostopoulou S, Kouladouros K, Piagkos G (2009) Eagle’s Syndrome: A Review of the Literature. Clin Anat 22: 545-558. [Crossref]
- Langlais RP, Miles DA, Van Dis ML (1986) Elongated and Mineralized Stylohyoid Ligament Complex: A Proposed Classification and Report of a Case of Eagle’s Syndrome. Oral Surg Oral Med Oral Pathol 61: 527-532. [Crossref]
- Correll RW, Jensen JL, Taylor JB, Rhyne RR (1979) Mineralization of the Stylohyoid- Stylomandibular Ligament Complex Incidence Study. Oral Surg Oral Med Oral Pathol 48: 286-291. [Crossref]
- Ilgüy M, Ilgüy D, Güler N Bayirli G (2005) Incidence of the Type and Calcification Patterns in Patients with Elongated Styloid Process. J Int Med Res 33: 96-102. [Crossref]
- Shaik MA, Naheeda, Kaleem SM, Wahab A, Hameed S (2013) Prevalence of Elongated Styloid Process in Saudi Population of Aseer Region. Eur J Dent 7: 449-454. [Crossref]
- Vieira EM, Guedes OA, Morais SD, Musis CR, Albuquerque PA et al. (2015) Prevalence of Elongated Styloid Process in a Central Brazilian Population. J Clin Diagn Res 9: ZC90-ZC92. [Crossref]
- Gracco A, De Stefani A, Bruno G, Balasso P, Alessandri-Bonetti G et al. (2017) Elongated Styloid Process Evaluation on Digital Panoramic Radiograph in a North Italian Population. J Clin Exp Dent 9: e400-e404. [Crossref]
- Zokaris N, Siska I, Natsis K, Piagkou M, Lazaridis N et al. (2019) Investigation of the Styloid Process Length in a Greek Population. Folia Morphol (Warsz) 78: 378-388. [Crossref]
- Eagle WW (1958) Elongated Styloid Process; symptoms and treatment. AMA Arch Otolaryngol 67:172-176. [Crossref]
- Pithon MM (2012) Eagle’s Syndrome in an Orthodontic Patient. Am J Orthod Dentofacial Orthop 141: 113-115. [Crossref]
- Taheri A, Firouzi-Marani S, Khoshbin M (2014) Nonsurgical Treatment of Stylohyoid (Eagle) Syndrome: A Case Report. J Korean Assoc Oral Maxillofac Surg 40: 246-249. [Crossref]
- Morrison PJ, Morrison RJ, McKinstry CS (2012) Familial Ossification of the Stylohyoid Ligament in a Three Generation Family - A New Clinical Entity Displaying Autosomal Dominant Inheritance. Br J Radiol 85: 458-459. [Crossref]
- Steinmann EP (1970) A New Light on the Pathogenesis of the Styloid Syndrome. Arch Otolaryngol 91: 171-174. [Crossref]
- Camarda AJ, Deschamps C, Forest D (1989) II. Stylohyoid Chain Ossification: A Discussion of Etiology. Oral Surg Oral Med Oral Pathol 67: 515-520. [Crossref]
- Tallgren A, Solow B (1987) Hyoid Bone Position, Facial Morphology and Head Posture in Adults. Eur J Orthod 9: 1-8. [Crossref]
- Adamidis IP, Spyropoulos MN (1992) Hyoid Bone Position and Orientation in Class I and Class III Malocclusions. Am J Orthod Dentofacial Orthop 101: 308-312. [Crossref]
- Baccetti T, Franchi L, McNamara JA (2005) The Cervical Vertebral Maturation (CVM) Method for the Assessment of Optimal Treatment Timing in Dentofacial Orthopedics. Seminars in Orthod 11: 119-129.
- de Andrade KM, Rodrigues CA, Watanabe PC, Mazzetto MO (2012) Styloid Process Elongation and Calcification in Subjects with TMD: Clinical and Radiographic Aspects. Braz Dent J 23: 443-450. [Crossref]
- Cançado RH, Lauris JRP (2014) Error of the Method: What Is It For? Dental Press J Orthod 19: 25-26. [Crossref]
- Koo TK, Li MY (2016) A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J Chiropr Med 15: 155-163. [Crossref]
- Nanjannawar L, Agrawal JÁ, Agrawal MS (2012) Pattern of Malocclusion and Treatment Need in Orthodontic Patients: An Institution-Based Study. World J Dentistry 3: 136-140.
- Willems G, De Bruyne I, Verdonck A, Fieuws S, Carels C (2001) Prevalence of Dentofacial Characteristics in a Belgian Orthodontic Population. Clin oral investig 5: 220-226. [Crossref]
- Piao Y, Kim SJ, Yu HS, Cha JY, Baik HS (2016) Five-Year Investigation of a Large Orthodontic Patient Population at a Dental Hospital in South Korea. Korean J Orthod 46: 137-145. [Crossref]
- Chandramani B More, Mukesh K Asrani (2010) Evaluation of the Styloid Process on Digital Panoramic Radiographs. Indian J Radiol Imaging 20: 261. [Crossref]
- Perkins JM, Subramanian SV, Davey Smith G, Özaltin E (2016) Adult Height, Nutrition, and Population Health. Nutr Rev 74: 149-165. [Crossref]