Prostate Cancer-Associated Trousseau´S Syndrome Versus Asymptomatic Isolated Muscular Calf Vein Thrombosis as the Origin of Acute Submassive Pulmonary Embolism: A Case Report and Review of the Literature
A B S T R A C T
Venous thromboembolism (VTE) is a major cause of morbidity and mortality in cancer patients. Cancer patients have a four to sevenfold increased risk of VTE compared with non-cancer patients and approximately 20% -30% of all VTE occurs in patients with cancer. Incidence of VTE varies with cancer type and is the highest among patients with metastatic-stage disease. Assessing risk of VTE in the patients with cancer and risk stratification tools as the Khorana score may predict VTE. The highest risk is associated with cancers of the pancreas, stomach, brain, and lung and some hematologic malignancies, whereas lower risks are associated with breast and prostate cancer. The incidence rate ratio (IRR) for prostate cancer is 3.25(2,56 - 4,13) and for pancreas 15.56 (10.50-23.0). We give a case report with a quite perplexing undertaking, where a submassive acute pulmonary embolism (PE) originated from an asymptomatic calf vein thrombosis or intertwined with the Trousseau´s syndrome.
Essential Section: One of the authors (A.T) was unexpected faced with the diagnosis of poorly differentiated prostate cancer. There were no signs of the disease, the PSA level was normal. As a retired medical oncologist, he had to care for many patients with prostate cancer and had now to cope with this cancer. To make the matter worse he suffered after the radical prostatectomy a submassive asymptomatic pulmonary embolism. Clinically there were no signs if a deep venous thrombosis. The coincidence of both events without clinical signs of a thrombosis could be caused by the Trousseau´s syndrome. Prostasomes extracellular vesicles synthesizes by prostate cancer cells and secreted into body fluids are prothrombotic by virtue of the expression of polyphosphate-activated coagulation factor XII.
Keywords
Venous thromboembolism (VTE), trousseau´s syndrome, prostate cancer, pulmonary embolisms, prostasomes, risk assessment
Case Presentation
Venous thromboembolism (VTE), comprising deep vein thrombosis (DVT) and pulmonary embolism (PE) is a major cause of morbidity and mortality in cancer patients. Cancer patients have a four to sevenfold increased risk of VTE compared with non-cancer patients and approximately 20% -30% of all VTE occurs in patients with cancer [1-8]. VTE is also a harbinger of cancer [9-15]. Prognosis of cancers associated with VTE and with an advanced stage of cancer is poor [11, 16, 17]. Symptomatic and incidental VTE are both associated with mortality in patients with prostate cancer [18-20]. The assessing risk of VTE in patient with cancer is of paramount importance and an essential component in diagnosis and therapy of the malignancy as published in the newest guidelines from ASCO and from ASH [21, 22]. The classical Virchow´s triad for the pathogenesis of VTE has now been supplemented and expanded by additional risk factors as genetic link between cancer and prognosis [23-25].
The risk factors for cancer-associated thrombosis are patient-specific factors as ethnicity, comorbidity (obesity, renal and pulmonary disease), female sex, heritable thrombophilia, prior history of VTE, cancer-specific factors as primary tumor site, histologic subtype, stage and grading, time from diagnosis, treatment-specific risk-factors as chemotherapy, hormonal therapy, antiangiogenic therapy, central venous catheters and Ports, supportive therapy with transfusions and Erythropoiesis-stimulating agents [26, 27]. The Khorana score for prediction of VTE and decision-making for thromboprophylaxis in cancer patients and has proven itself very well in the clinic as it is shown in (Figure 1) [28-30].
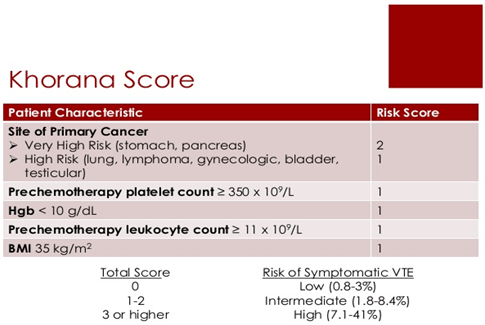
Figure 1: Khorana-Score: A predictive model clinical risk score for VTE.
BMI= body mass index [28-30].
Prostate cancer does not belong to the high-risk entities for VTE as gastric and pancreas cancer. The initial incidence rate ratio (IRR) for prostate cancer is 3.25 (2.56 - 4.13) whereas for pancreas cancer the IRR is 15.56 (10.50 - 23.06) [8, 31, 32]. The association between VTE and malignancy was first described in 1865 by Armand Trousseau [33-35]. Since its discovery, the association of cancer and VTE is often termed Trousseau´s syndrome. Despite its frequent mention in reviews the term Trousseau´s syndrome is not in the MESH headings of Medline or PubMed [7, 33, 34, 36-39]. Literature searching using Boole´s operator Prostate cancer and Trousseau´s syndrome and Thromboembolic disease did not result in PubMed. So far, the literature on the role of hemostasis in genitourinary malignancies -prostate, bladder and kidney cancer- and VTE is quite scant. A recent review on the role of the coagulation system in genitourinary cancers summarizes the pathophysiology of coagulation activation and the underlying molecular mechanisms and gives no clue for the Trousseau´s syndrome [40].
One of the authors (A. Ts.), 73-years-old, turned up in our clinic in January 2020 for clarification of prostate cancer. Except for medicated type of high blood pressure, the patient did not have severe diseases, a prior history of VTE or cancer and there is no family history of prostate nor related cancers. A diagnostic work-up was started with multiparametric MRI (mpMRI) [41-43]. In the peripheral zone right-dorsal a PI-RADS 4-lesion within the organ and a PI-RADS 3-lesion in the transition zone were detected. The MRI-targeted systematic and combined biopsies of the prostate by the transperineal approach were performed in the same month [44, 45]. From the 17 biopsies incl. both with PI-RADS 3 and PI-RADS-4, 6 showed histopathologically an aciniform adenocarcinoma of the prostate with Gleason-score 5+5=10.
The prostate-specific antigen level (PSA) was < 4.0ng per milliliter [46, 47]. For the completion for the primary staging a 68Ga-PSMA-PET/CT was carried out on 11th January 2020 [48-50]. The fused PET/CT showed intense prostate-specific membrane antigen (PSMA) expression confined strictly to the prostate, without PSMA-positive lymph nodes and without metastasis to organs. On 06/03/2020 the daVinci-robot-assisted radical prostatectomy was conducted by one of the co-authors (Prof. J. Roigas) under the usual standard precautions [51-53]. The patient received a prophylactic anticoagulation with LMWH according to the guidelines [21, 22]. The postoperative course was unremarkable. The patient was mobilized and under the supervision of a physiotherapist the patient walked and could also walk stairs. From the third day on he noticed a tinge of blood in his sputum. An otoscopic endoscopic examination revealed no source of bleeding. The patient had no cough, no fever and no swellings of the legs.
From the fourth to the fifth day on he developed slightly increased temperature < 38°C. He had no shortness of breath and no pain. On 13/03/2020 the temperature was measured at 39°C on several occasions during this day. On the same day computed tomography (CT) of thorax and abdomen revealed a multisegmental pulmonary embolism in the middle and in right lower lobe. In the left lower lobe was a pneumonic inflammatory infiltration most likely to be considered as pulmonary infarction [54, 55]. The colour Doppler study disclosed an isolated muscular soleal vein thrombosis of the left lower leg [56, 57]. The deep veins were open. Echocardiography from 17/03/2020 did not reveal right heart failure and showed a ventricular ejection fraction of 60%. Blood and urine culture were negative for pathogenic microbes. In the meantime, the dosis of the LMWH was increased and an i.v- antibiosis with Tazobactam (Tazobac®) 3 x 4.5g was initiated [58-61]. Under this therapy the fever was quickly resolved, and the patient was released on 19/03/2020. The anticoagulation was switched to an oral Factor Xa-inhibitor - Endoxaban (Lixiana®) 60 mg/die [60-65].
For the critical appraisal whether the acute submassive and asymptomatic pulmonary embolism has its origin in the isolated thrombosis of muscular soleal vein of the left calf, or is a complication of the surgical procedure or last but not least an indication of Trousseau´s syndrome due to circulating prostasomes [20, 37, 40, 57, 66-71]. Biomarkers for the prediction of VTE in cancer in the era of “ personalized medicine” are plentiful and have to be validated and tested [40, 72-76]. As it was introduced for tumor markers with the tumor marker utility grading system (TMUGS) a similar system for biomarker for prediction of VTE in cancer would be of great help [73, 77, 78]. Very few biomarker tests for VTE prediction have passed these high bars for routine clinical application [76, 79]. The Khorana VTE risk assessment score and the Vienna VTE risk assessment score are scores not specified for prostate cancer [75, 80]. Therefore, there is an urgent need for the development of a VTE risk assessment score for prostate cancer. We hypothesize that prostasomes could function as a source of diagnostic biomarkers for prostate cancer [37, 70, 71, 81-84]. These extracellular vesicles (also termed exosomes) are synthesized in prostate cancer cells and secreted into body fluids [85]. Prostasome are prothrombotic by virtue of the expression of polyphosphate-activated coagulation factor XII, which initiates coagulation through the extrinsic pathway [37, 69]. Tavoosidana et al. demonstrated in box plots plasma levels of prostasomes according to histological Gleason score. The level of prostasomes were significantly elevated in the highest Gleason score [70]. The measurement of prostasomes in peripheral blood may be useful for early diagnosis and assessment of prognosis in organ-confined prostate cancer and for VTE risk assessment. In October 2018, a clinical trial was launched under the title “ Prostasomes as Diagnostic Tool for Prostate Cancer Detection” under the Clinical Trials. Gov Identifier: NCT03694483 which is still recruiting and the estimated primary completion date is October 1, 2023. - link. Among others, it was shown that prostasomes are associated with VTE independently from the Gleason score. Just recently an ASCO guideline on “ Molecular biomarkers in localized prostate cancer” was released with a special emphasis on commercially available multigene expression classifier[86]. As listed in the patient-specific factors for cancer-associated VTE thrombophilia may be associated with VTE [87-89]. The diagnostic workup includes thrombophilia testing as Factor V Leiden, prothrombin 20210A, Lupus anticoagulants and MTHFR.
The final histopathological result of the patient was: pT2c, pN0, pN0, 0pL0, pV0, R0, Gleason-score 5+4=9. The radical prostatectomy with the histopathological result is no indication for an adjuvant therapy [90]. The clinical outcome for patients with a Gleason score 9-10 prostate adenocarcinoma and in men with organ-confined margin-negative disease had a very low risk of early biochemical recurrence [91-93]. Therefore, after radical prostatectomy with the histopathological results as mentioned above, there is no indication for an adjuvant therapy according to ESMO and NCCN guidelines [90, 94].
The cancer statistics, 2020 and their survival statistics show that prostate cancer belongs to the entities with the highest 5-year survival rates ( 98%) as melanoma of the skin (92%) and female breast cancer ( 90%) [95].
Competing Interest
None.
Author Contributions
A. Ts. performed the literature search, A. G. , S. G, and J. R and A. T. conceived, wrote, edited, and approved the manuscript.
Article Info
Article Type
Case Report and Review of the LiteraturePublication history
Received: Wed 22, Apr 2020Accepted: Tue 05, May 2020
Published: Tue 12, May 2020
Copyright
© 2023 Antonis Tsamaloukas. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.COR.2020.05.05
Figures & Tables
BMI= body mass index [28-30].
References
- Al Samkari H, AB Song, JM Connors (2020) Cancer-associated thrombosis: Where do we stand? ADVANCES IN CELL AND GENE THERAPY 3: e73.
- Buller HR, van Doormaal FF, van Sluis GL, Kamphuisen PW (2007) Cancer and thrombosis: from molecular mechanisms to clinical presentations. J Thromb Haemost 5: 246-254. [Crossref]
- Chew HK, Wun T, Harvey D, Zhou H, White RH (2006) Incidence of Venous Thromboembolism and Its Effect on Survival Among Patients with Common Cancers. Arch Intern Med 166: 458-464. [Crossref]
- Cohen AT, Katholing A, Rietbrock S, Bamber L, Martinez C (2017) Epidemiology of first and recurrent venous thromboembolism in patients with active cancer. Thromb Haemost 26: 57-65. [Crossref]
- Donnellan E, Khorana AA (2017) Cancer and Venous Thromboembolic Disease: A Review. Oncologist 22: 199-207. [Crossref]
- Alok A Khorana (2012) Cancer and coagulation. Am J Hematol 87: S82-S87. [Crossref]
- Prandoni P, Falanga A, Piccioli A (2005) Cancer and venous thromboembolism. Lancet Oncol 6: 401-410. [Crossref]
- Streiff MB (2016) Thrombosis in the setting of cancer. Hematology Am Soc Hematol Educ Program 2016: 196-205. [Crossref]
- Carrier M, Lazo-Langner A, Shivakumar S, Tagalakis V, Zarychanski R et al. (2015) Screening for Occult Cancer in Unprovoked Venous Thromboembolism. N Engl J Med 373: 697-704. [Crossref]
- Monreal M, Lafoz E, Casals A, Inaraja L, Montserrat E et al. (1991) Occult cancer in patients with deep venous thrombosis. A systematic approach. Cancer 67: 541-545. [Crossref]
- Sørensen HT, Mellemkjaer L, Olsen JH, Baron JA (2000) Prognosis of Cancers Associated with Venous Thromboembolism. N Engl J Med 343: 1846-1850. [Crossref]
- Khorana AA (2019) If Trousseau had a stroke. Blood 133: 769-770. [Crossref]
- Navi BB, Reiner AS, Kamel H, Iadecola C, Okin PM et al. (2019) Arterial thromboembolic events preceding the diagnosis of cancer in older persons. Blood 133: 781-789. [Crossref]
- White RH, Chew HK, Zhou H, Parikh-Patel A, Harris D et al. (2005) Incidence of Venous Thromboembolism in the Year Before the Diagnosis of Cancer in 528 693 Adults. Arch Intern Med 165: 1782-1787. [Crossref]
- Robertson L, Yeoh SE, Broderick C, Stansby G, Agarwal R (2018) Effect of testing for cancer on cancer- or venous thromboembolism (VTE)-related mortality and morbidity in people with unprovoked VTE. Cochrane Database Syst Rev 11: CD010837. [Crossref]
- Kuderer NM, Ortel TL, Francis CW (2009) Impact of Venous Thromboembolism and Anticoagulation on Cancer and Cancer Survival. J Clin Oncol 27: 4902-4911. [Crossref]
- Timp JF, Braekkan SK, Versteeg HH, Cannegieter SC (2013) Epidemiology of cancer-associated venous thrombosis. Blood 122: 1712-1723. [Crossref]
- Chaturvedi S, Sidana S, Elson P, Khorana AA, McCrae KR (2014) Symptomatic and incidental venous thromboembolic disease are both associated with mortality in patients with prostate cancer. PLoS One 9: e94048. [Crossref]
- Van Hemelrijck M, Adolfsson J, Garmo H, Bill-Axelson A, Bratt O et al. (2010) Risk of thromboembolic diseases in men with prostate cancer: results from the population-based PCBaSe Sweden. Lancet Oncol 11: 450-458. [Crossref]
- Tyritzis SI, Wallerstedt A, Steineck G, Nyberg T, Hugosson J et al. (2015) Thromboembolic Complications in 3,544 Patients Undergoing Radical Prostatectomy with or without Lymph Node Dissection. J Urol 193: 117-125. [Crossref]
- Key NS, Khorana AA, Kuderer NM, Bohlke K, Lee AYY et al. (2020) Venous Thromboembolism Prophylaxis and Treatment in Patients with Cancer: ASCO Clinical Practice Guideline Update. J Clin Oncol 38: 496-520. [Crossref]
- Anderson DR, Morgano GP, Bennett C, Dentali F, Francis CW et al. (2019) American Society of Hematology 2019 guidelines for management of venous thromboembolism: prevention of venous thromboembolism in surgical hospitalized patients. Blood Adv 3: 3898-3944. [Crossref]
- Dickson BC (2004) Venous thrombosis: on the history of Virchow’s triad. Univ Toronto Med J 81: 166-171.
- Boccaccio C, Comoglio PM (2009) Genetic link between cancer and thrombosis. J Clin Oncol 27: 4827-4833. [Crossref]
- Morange PE, Suchon P, Trégouët DA (2015) Genetics of Venous Thrombosis: update in 2015. Thromb Haemost 114: 910-919. [Crossref]
- Khorana AA, Francis CW, Culakova E, Kuderer NM, Lyman GH Frequency, risk factors, and trends for venous thromboembolism among hospitalized cancer patients. Cancer 110: 2339-2346. [Crossref]
- Menapace LA, Khorana AA (2010) The role of thromboprophylaxis in cancer patients: emerging data. Curr Opin Hematol 17: 450-456. [Crossref]
- Khorana AA, Connolly GC (2009) Assessing Risk of Venous Thromboembolism in the Patient with Cancer. J Clin Oncol 27: 4839-4847. [Crossref]
- Kuderer NM, Culakova E, Lyman GH, Francis C, Falanga A et al. (2016) A Validated Risk Score for Venous Thromboembolism Is Predictive of Cancer Progression and Mortality. Oncologist 21: 861-867. [Crossref]
- Mulder FI, Candeloro M, Kamphuisen PW, Di Nisio M, Bossuyt PM et al. (2019) The Khorana score for prediction of venous thromboembolism in cancer patients: a systematic review and meta-analysis. Haematologica 104: 1277-1287. [Crossref]
- Blom JW, Doggen CJ, Osanto S, Rosendaal FR (2005) Malignancies, Prothrombotic Mutations, and the Risk of Venous Thrombosis. JAMA 293: 715-722. [Crossref]
- Walker AJ, Card TR, West J, Crooks C, Grainge MJ (2013) Incidence of venous thromboembolism in patients with cancer-a cohort study using linked United Kingdom databases. Eur J Cancer 49: 1404-1413. [Crossref]
- Rickles FR, Edwards RL (1983) Activation of blood coagulation in cancer: Trousseau's syndrome revisited. Blood 62: 14-31. [Crossref]
- Varki A (2007) Trousseau's syndrome: multiple definitions and multiple mechanisms. Blood 110: 1723-1729. [Crossref]
- Khorana AA (2003) Malignancy, thrombosis and Trousseau: the case for an eponym. J Thromb Haemost 1: 2463-2465. [Crossref]
- Ikushima S, Ono R, Fukuda K, Sakayori M, Awano N et al. (2016) Trousseau's syndrome: cancer-associated thrombosis. Jpn J Clin Oncol 46: 204-208. [Crossref]
- Key NS (2015) New players in Trousseau syndrome. Blood 126: 1270-1272. [Crossref]
- Stolinsky DC (1983) Trousseau's phenomenon. Blood 62: 1304. [Crossref]
- Ogren M, Bergqvist D, Wåhlander K, Eriksson H, Sternby NH (2006) Trousseau's syndrome - what is the evidence? A population-based autopsy study. Thromb Haemost 95: 541-545. [Crossref]
- John A, Gorzelanny C, Bauer AT, Schneider SW, Bolenz C (2017) Role of the Coagulation System in Genitourinary Cancers: Review. Clin Genitourin Cancer S1558-7673: 30210. [Crossref]
- Stabile A, Giganti F, Rosenkrantz AB, Taneja SS, Villeirs G et al. (2020) Multiparametric MRI for prostate cancer diagnosis: current status and future directions. Nat Rev Urol 17: 41-61. [Crossref]
- Turkbey B, Brown AM, Sankineni S, Wood BJ, Pinto PA et al. (2016) Multiparametric prostate magnetic resonance imaging in the evaluation of prostate cancer. CA Cancer J Clin 66: 326-336. [Crossref]
- Turkbey B, Rosenkrantz AB, Haider MA, Padhani AR, Villeirs G et al. (2019) Prostate imaging reporting and data system version 2.1: 2019 update of prostate imaging reporting and data system version 2. Eur Urol 76: 340-351 [Crossref]
- Ahdoot M, Wilbur AR, Reese SE, Lebastchi AH, Mehralivand S et al. (2020) MRI-Targeted, Systematic, and Combined Biopsy for Prostate Cancer Diagnosis. N Engl J Med 382: 917-928. [Crossref]
- Pesapane F, Standaert C, De Visschere P, Villeirs G (2020) T-staging of prostate cancer: Identification of useful signs to standardize detection of posterolateral extraprostatic extension on prostate MRI. Clin Imaging 59: 1-7. [Crossref]
- Carter HB (2004) Prostate Cancers in Men with Low PSA Levels — Must We Find Them? N Engl J Med 350: 2292-2294. [Crossref]
- Thompson IM, Pauler DK, Goodman PJ, Tangen CM, Lucia MS et al. (2004) Prevalence of Prostate Cancer among Men with a Prostate-Specific Antigen Level ≤4.0 ng per Milliliter. N Engl J Med 350: 2239-2246. [Crossref]
- Maurer T, Eiber M, Schwaiger M, Gschwend JE (2016) Current use of PSMA–PET in prostate cancer management. Nat Rev Urol 13: 226-235. [Crossref]
- Perera M, Papa N, Christidis D, Wetherell D, Hofman MS et al. (2016) Sensitivity, specificity, and predictors of positive 68Ga–prostate-specific membrane antigen positron emission tomography in advanced prostate cancer: a systematic review and meta-analysis. Eur Urol 70: 926-937. [Crossref]
- Hofman MS, Lawrentschuk N, Francis RJ, Tang C, Vela I et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): a prospective, randomised, multi-centre study. Lancet 395: 1208-1216. [Crossref]
- Costello AJ (2020) Considering the role of radical prostatectomy in 21st century prostate cancer care. Nat Rev Urol 17: 177-188. [Crossref]
- Humphreys MR, Gettman MT, Chow GK, Zincke H, Blute ML (2004) Minimally invasive radical prostatectomy. Mayo Clin Proc 79:1169-1180. [Crossref]
- El-Hakim A, Leung RA, Tewari A (2006) Robotic prostatectomy: a pooled analysis of published literature. Expert Rev Anticancer Ther 6: 11-20. [Crossref]
- Sista AK, Kuo WT, Schiebler M, Madoff DC (2017) Stratification, Imaging, and Management of Acute Massive and Submassive Pulmonary Embolism. Radiology 284: 5-24. [Crossref]
- Wittram C, Maher MM, Yoo AJ, Kalra MK, Shepard JA et al. (2004) CT Angiography of Pulmonary Embolism: Diagnostic Criteria and Causes of Misdiagnosis. Radiographics 24: 1219-1238. [Crossref]
- Caggiati A, Bergan JJ, Gloviczki P, Eklof B, Allegra C et al. (2005) Nomenclature of the veins of the lower limb: Extensions, refinements, and clinical application. J Vasc Surg 41: 719-724. [Crossref]
- Galanaud JP, Sevestre MA, Genty C, Laroche JP, Zizka V et al. (2010) Comparison of the clinical history of symptomatic isolated muscular calf vein thrombosis versus deep calf vein thrombosis. J Vasc Surg 52: 932-938. [Crossref]
- Becattini C, Agnelli G (2020) Acute treatment of venous thromboembolism. Blood 135: 305-316. [Crossref]
- Konstantinides SV, Meyer G, Becattini C, Bueno H, Geersing GJ et al. (2019) 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS): The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). Eur Heart J 41: 543-603. [Crossref]
- Lee AYY (2020) Anticoagulant Therapy for Venous Thromboembolism in Cancer. N Engl J Med 382: 1650-1652. [Crossref]
- Moik F, Pabinger I, Ay C (2020) How I treat cancer-associated thrombosis. ESMO Open 5: e000610. [Crossref]
- Ay C, Beyer-Westendorf J, Pabinger I (2019) Treatment of cancer-associated venous thromboembolism in the age of direct oral anticoagulants. Ann Oncol 30: 897-907. [Crossref]
- Elizabeth Bowhay-Carnes, Anand Karnad, Subrata Haldar, John Sarantopoulos, Sumit Madan (2015) Role of NovelAnticoagulants in Primary and Secondary Thromboprophylaxis in Cancer. J Hematol Thromboembol Dis 3.
- Kearon C, Kahn SR (2020) Long-term treatment of venous thromboembolism. Blood 135: 317-325. [Crossref]
- Raskob GE, van Es N, Verhamme P, Carrier M, Di Nisio M et al. (2017) Edoxaban for the Treatment of Cancer-Associated Venous Thromboembolism. N Engl J Med 378: 615-624. [Crossref]
- Rice KR, Brassell SA, McLeod DG (2010) Venous thromboembolism in urologic surgery: prophylaxis, diagnosis, and treatment. Rev Urol 12: e111-e124. [Crossref]
- Schmitges J, Trinh QD, Sun M, Abdollah F, Bianchi M et al. (2012) Venous thromboembolism after radical prostatectomy: the effect of surgical caseload. BJU Int 110: 828-833. [Crossref]
- Sofra M, Antenucci A, Gallucci M, Mandoj C, Papalia R et al. (2014) Perioperative changes in pro and anticoagulant factors in prostate cancer patients undergoing laparoscopic and robotic radical prostatectomy with different anaesthetic techniques. J Exp Clin Cancer Res 33: 63. [Crossref]
- Nickel KF, Ronquist G, Langer F, Labberton L, Fuchs TA et al. (2015) The polyphosphate–factor XII pathway drives coagulation in prostate cancer-associated thrombosis. Blood 126: 1379-1389. [Crossref]
- Tavoosidana G, Ronquist G, Darmanis S, Yan J, Carlsson L et al. (2011) Multiple recognition assay reveals prostasomes as promising plasma biomarkers for prostate cancer. Proc Natl Acad Sci U S A 108: 8809-8814. [Crossref]
- Zijlstra C, Stoorvogel W (2016) Prostasomes as a source of diagnostic biomarkers for prostate cancer. J Clin Invest 126: 1144-1151. [Crossref]
- Hanna DL, White RH, Wun T (2013) Biomolecular markers of cancer-associated thromboembolism. Crit Rev Oncol Hematol 88: 19-29. [Crossref]
- Hayes DF (2015) Biomarker validation and testing. Mol Oncol 9: 960-966. [Crossref]
- Mahajan A, Wun T (2019) Biomarkers of Cancer-Associated Thromboembolism. Cancer Treat Res 179: 69-85. [Crossref]
- Pabinger I, Thaler J, Ay C (2013) Biomarkers for prediction of venous thromboembolism in cancer. Blood 122: 2011-2018. [Crossref]
- Romero Otero J, Garcia Gomez B, Campos Juanatey F, Touijer KA (2014) Prostate cancer biomarkers: An update. Urol Oncol 32: 252-260. [Crossref]
- Hayes DF (2009) Clinical Utility of Tumor Markers: Study Design and Evaluation 273-277. [Crossref]
- Hayes DF, Bast RC, Desch CE, Fritsche H Jr, Kemeny NE et al. (1996) Tumor Marker Utility Grading System: a Framework to Evaluate Clinical Utility of Tumor Markers. J Natl Cancer Inst 88: 1456-1466. [Crossref]
- Dijkstra S, Mulders PF, Schalken JA (2014) Clinical use of novel urine and blood based prostate cancer biomarkers: A review. Clin Biochem 47: 889-896. [Crossref]
- Khorana AA, Kuderer NM, Culakova E, Lyman GH, Francis CW (2008) Development and validation of a predictive model for chemotherapy-associated thrombosis. Blood 111: 4902-4907. [Crossref]
- Oral contraceptives and venous thromboembolic disease, surgically confirmed gallbladder disease, and breast tumours. Report from the Boston Collaborative Drug Surveillance Programme. (1973) Lancet 1: 1399-404. [Crossref]
- Smits M, Mehra N, Sedelaar M, Gerritsen W, Schalken JA (2017) Molecular biomarkers to guide precision medicine in localized prostate cancer. Exp Rev Mol Diagn 17: 791-804. [Crossref]
- Hendriks R, I Van Oort, J Schalken (2017) Blood-based and urinary prostate cancer biomarkers: a review and comparison of novel biomarkers for detection and treatment decisions. Prostate Cancer Prostatic Dis 20: 12-19. [Crossref]
- Boerrigter E Groen LN, Van Erp NP, Verhaegh GW, Schalken JA (2020) Clinical utility of emerging biomarkers in prostate cancer liquid biopsies. Exp Rev Mol Diagn 20: 219-230. [Crossref]
- Gurunathan S, Kang MH, Jeyaraj M, Qasim M, Kim JH (2019) Review of the Isolation, Characterization, Biological Function, and Multifarious Therapeutic Approaches of Exosomes. Cells 8: E307. [Crossref]
- Eggener SE, Rumble RB, Armstrong AJ, Morgan TM, Crispino T et al. (2020) Molecular Biomarkers in Localized Prostate Cancer: ASCO Guideline. J Clin Oncol 38: 1474-1494. [Crossref]
- Connors JM (2017) Thrombophilia Testing and Venous Thrombosis. N Engl J Med 377: 1177-1187. [Crossref]
- Kennedy M, Andreescu AC, Greenblatt MS, Jiang H, Thomas CA et al. (2005) Factor V Leiden, prothrombin 20210A and the risk of venous thrombosis among cancer patients. Br J Haematol 128: 386-388. [Crossref]
- Pabinger I, Ay C, Dunkler D, Thaler J, Reitter EM et al. (2015) Factor V Leiden mutation increases the risk for venous thromboembolism in cancer patients – results from the Vienna Cancer And Thrombosis Study (CATS). J Thromb Haemost 13: 17-22. [Crossref]
- Parker C, Gillessen S, Heidenreich A, Horwich A; ESMO Guidelines Committee (2015) Cancer of the prostate: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 26: v69-v77. [Crossref]
- Fischer S, Lin D, Simon RM, Howard LE, Aronson WJ et al. (2016) Do all men with pathological Gleason score 8–10 prostate cancer have poor outcomes? Results from the SEARCH database. BJU Int 118: 250-257. [Crossref]
- Kishan AU, Cook RR, Ciezki JP, Ross AE, Pomerantz MM et al. (2018) Radical Prostatectomy, External Beam Radiotherapy, or External Beam Radiotherapy With Brachytherapy Boost and Disease Progression and Mortality in Patients With Gleason Score 9-10 Prostate Cancer. JAMA 319: 896-905. [Crossref]
- Sandler KA, Cook RR, Ciezki JP, Ross AE, Pomerantz MM et al. (2018) Clinical Outcomes for Patients With Gleason Score 10 Prostate Adenocarcinoma: Results From a Multi-institutional Consortium Study. Int J Radiat Oncol Biol Phys 101: 883-888. [Crossref]
- Mohler JL, Antonarakis ES, Armstrong AJ, D'Amico AV, Davis BJ et al. (2019) Prostate Cancer, Version 2.2019, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 17: 479-505. [Crossref]
- Siegel RL, Miller KD, Jemal A (2020) Cancer statistics, 2020. CA Cancer J Clin 70: 7-30. [Crossref]