Prospective Clinical Investigation of Orthodontic Relapse from Gingival Clefts
A B S T R A C T
Background: Orthodontic space closure following premolar extraction may result in gingival cleft formation. This may contribute to orthodontic relapse due to reopening of extraction spaces.
Purpose: 1) To see the effects gingival clefts have on relapse and opening of closed extraction spaces after orthodontic treatment. 2) To record any changes in cleft severity that may occur. 3) To evaluate any relationship between gingival phenotype and cleft severity.
Methods: Subjects recruited from previous study in which gingival clefts were measured during space closure. The clinical measures included the occurrence and severity of clefts and their relationship to gingival phenotype.
Results: Sites with a cleft (N=42) had 42.86% relapse and those without (N=19) had 36.84% relapse.
Conclusions: As gingival cleft severity increases, the amount of relapse distance is likely to increase. Patients with a thick gingival phenotype who obtain gingival clefts in extraction sites during orthodontic treatment are more likely to have relapse post-treatment compared to sites which did not develop a gingival cleft.
Keywords
Gingival clefts, orthodontic relapse, retention
Introduction
Premolar extraction followed by space closure mechanics is common practice in orthodontics treatment [1]. A consequence of moving teeth to close space is the formation of an invagination in the gingiva, which is also called a gingival cleft [2-4]. These gingival clefts may delay or even prevent space closure, as well as contribute to relapse of closed extraction spaces after orthodontic treatment is completed [5, 6]. In 1983 Rivera Circuns mentions that these invaginations can vary from a minor one surface crease in the attached gingiva to a deep cleft that extends across the interdental papilla from the buccal to the lingual alveolar surface [7].
When looking at the periodontium, the most common occurring changes in orthodontic extraction cases are gingival recession, gingival overgrowth, and gingival invaginations (Figure 1). [2, 8]. Due to the compression and retraction forces at sites of extraction the interdental papillae may enlarge and accumulate resulting in gingival invaginations [9, 10]. Previous investigations showed that when teeth were not treated with surgical resection of the cleft, the tension side fibers were subject to considerable stress while the compression side fibers had a “coiled” appearance [11, 12]. It was noted that transeptal fibers are probably the major cause of relapse because of their soft tissue attachments which offer no adjustment of distorted fibers [11].
A study conducted by Edwards observed any relapse in extraction areas during a 12-18-month period post-orthodontic treatment. In ten instances, where surgical intervention was used to remove excess gingival tissue, the gingival groove remained in four of the cases [5]. However, the grooves did not extend into the interproximal papilla as was previously observed in these areas. In all cases, a healthy interdental papilla resulted with no abnormalities in adaptation to the adjacent teeth. This suggests that the bunched up (folded) excess tissue does play a pertinent role in the reopening of extraction sites because of the noticeable success in reducing the relapse of approximated teeth by surgical removal of this tissue. Transeptal fibers were not surgically removed in this study, and since the histology evidence showed little morphologic distortion in transeptal regions (during the 12-18-month retention phase), it can be assumed that some mechanism does exist which is able to reorganize these supporting transeptal fibers after orthodontic space closure. Parker saw that the stability of retracted teeth was increased with paralleled tooth roots [11]. When teeth were tipped together, the relapse rate averaged 42% [13].
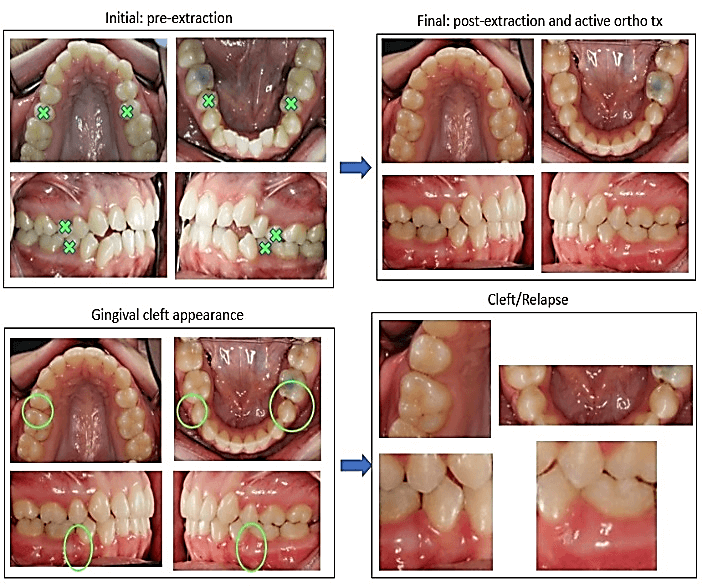
Figure 1: Study subject, Photographs of subject prior to extractions, post-extractions/post-orthodontic treatment, magnified photographs post-treatment.
However, when the roots were parallel the rates averaged 13% [11]. Parker found that when surgical intervention was used along with orthodontic retention this had a positive effect on stability of retracted teeth, in fact, the teeth moved further into extraction sites [11]. A previous study undertaken in the Department of Orthodontics at the University of Maryland investigated the gingival cleft formation from premolar extractions and subsequent space closure, resulting in an overall incidence of 71.4% [14]. The premolar extraction sites were measured for soft tissue and bone parameters to determine a correlation between the gingival phenotype and cleft formation.
Thus, in our current follow-up study we are able to utilize pre-existing data of the study subjects pertaining to cleft formation and cleft volume based on their gingival phenotypes. Having a data base of these subject’s gingival phenotypes present at the extraction site allows for comparison of changes based on these parameters. The objectives of this study were to investigate gingival clefts and the effects they have on relapse and re-opening of extraction spaces after orthodontic treatment, to record any changes in cleft severity that may occur over time, and to evaluate any relationship between gingival phenotype and cleft severity. The outcome of this current study can help orthodontists make an informed decision on the type of retention they are going to prescribe and whether it may be more beneficial to excise the gingival cleft to avoid any associated relapse. We want to know if gingival invaginations can affect the stability and retention of treatment and if it does, which group of patients are more affected.
Materials and Methods
I Subjects
Subjects were recruited from a preceding study done at the University of Maryland orthodontic clinic [14]. Forty-two subjects completed that study (17 males, 25 females) with 91 premolar extraction sites being measured for the incidence of gingival clefts, gingival cleft severity, and gingival thickness in premolar extraction sites all while in orthodontic treatment. Eighteen subjects (7 male and 11 female) of the original 42 were measured in this current study consisting of 61 extraction sites with measurements. These sites were measured only after removal of fixed appliances. The other 24 did not participate because they had not finished orthodontic treatment while measurements were being made. Consent/assent and HIPAA authorization forms were reviewed with patient/guardian.
II Data Collection
In these subjects which underwent orthodontic treatment with extractions of at least two premolars followed by space closure, measurements were made consisting of: relapse space, current gingival cleft dimensions, cleft severity, and keratinized gingiva. Measurements in these categories were made three individual times by the same recorder at each visit to account for possible errors made with each measurement. The mean of the three recordings was then used as that day’s measurement. Retention check protocol in the department of orthodontics at the University of Maryland consists of the following interval: on the day of debond, 1-month post debond (into retention), 3 months into retention, 6 months into retention, and 1 year into retention. Subject measurements were scheduled to take place at these five intervals, however, due to the complexity of scheduling patients in a University clinic setting, the majority of subjects were measured three to four times for this study. The experimental sites had a cleft present at the extraction location during the preceding investigation, while the control sites had an absence of a gingival cleft at the extraction site during the preceding investigation.
The severity of clefts was assessed by measurements using Reichert’s coding system: (Reichert et al. 2011) the same system used to measure cleft severity in the preceding investigation [15]. Soft tissue measurements were taken in three planes using a Maryland (Moffitt) periodontal probe
i. Mesial-distal (x-axis dimension).
ii. Bucco-lingual (y-axis dimension) (Figure 2).
iii. Occlusal-gingival (z-axis dimension) (Figure 3).
Figure 2: Original drawing of a measurement in the bucco-lingual dimension.
Figure 3: Original drawing of a measurement in the occlusal-gingival dimension.
Measurements were made in the x, y, and z planes to determine gingival cleft severity. Figure 4 demonstrates a gingival cleft between the upper right second premolar and canine with the periodontal probe just outside of the cleft. Figure 5 Illustrates the same site with the periodontal probe inside the cleft in the Z direction (occlusal-gingival). Figure 6 Illustrates probing depth of the gingival cleft in the Y direction (bucco-lingual).
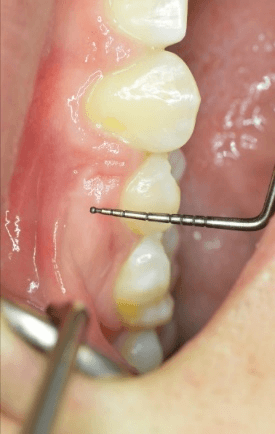
Figure 4: Gingival cleft next to periodontal probe.
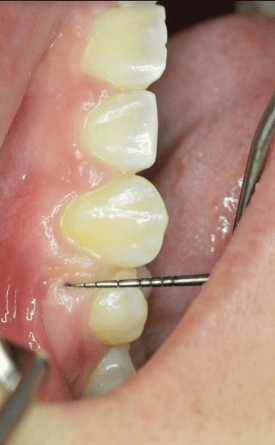
Figure 5: Gingival cleft with periodontal probe in Z direction.
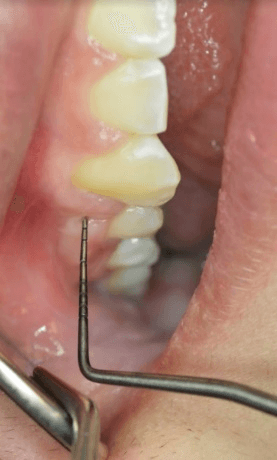
Figure 6: Gingival cleft with periodontal probe in Y direction.
The degree of severity was determined by the volumetric equation:
Severity=(x)^2+(y)^2+(z)^2
The mesial-distal measurement for each subject’s gingival cleft was determined by the width of the periodontal probe at which the bucco-lingual measurement was made. An electronic digital caliper was used to measure the width of the periodontal probe:
Hu-Friedy PCPMDBIU
Measurements found in APPENDIX A
The width of any extraction space relapse was measured between the adjacent teeth using an IPR thickness gauge (Align Space Gauge Set, Align Technology, San Jose, CA) (Figure 7). The IPR gauges had measurements of 0.1mm, 0.2mm, 0.25mm, 0.3mm, 0.4mm, 0.5mm. Any space measured where the 0.1mm gauge could not fit was recorded as 0mm.

Figure 7: Align Space Gauge Set.
The type of retention appliance used by each subject was recorded.
III Statistical Methods
Sites were divided up into subgroups defined by predictor variables: gingival phenotype, relapse, amount of relapse, cleft severity, and presence of a previous cleft. These groups were compared to each other using Spearman’s rank order correlation. This statistical analysis was used to summarize the strength and direction between variables, and to find any statistically significant positive or negative correlations resulting from them.
Results
Of the 61 sites measured, 42 entered the study with a cleft (experimental sites) and 19 (control sites) did not have a cleft. Seven of the 19 controls had relapse (36.84%), 18 of the 42 experimental sites had relapse (42.86%). Of all the sites there was a total relapse of 40.98% (Table 1). Some of the sites had an initial measurement (at day of debond) greater than 0mm, meaning space was not completely closed during active orthodontic treatment. For the purpose of this study, relapse/space reopening was determined when the final measurement was greater than the initial measurement.
Table 1: Control vs. Experimental Data.
|
Controls vs. Experimental |
||
|
# Controls (n=19) with Relapse |
# Experimental (n=42) with Relapse |
Total # (n=61) with Relapse |
|
7 (36.84%) |
18 (42.86%) |
25 (40.98%) |
The average reopening space was 0.128mm with a range of 1.8mm having a minimum of -0.3mm and maximum of 1.5mm. The relapse median and mode were both 0mm.
I Severity
At the completion of this study's measurements, 25 sites had a cleft severity of 0 mm2 in which 7 (28%) had relapse (Table 2). 21 sites had a cleft severity greater than 0 mm2 and less than or equal to 15 mm2, and 10 of these (47.62%) had relapse. 11 sites had a cleft severity greater than 15 mm2 and less than or equal to 30 mm2, and 6 (54.55%) of these had relapse. 4 sites had a cleft severity greater than 30 mm2 and 2 (50%) had relapse. An overall mean gingival cleft severity of 18.47 mm2 was found as well.
Table 2: Severity Data.
|
Cleft Severity (mm2) with Relapse |
|||||
|
# Sites with Cleft Severity of 0 (n=25) which had Relapse |
# Sites with Cleft Severity >0 and ≤15 (n=21) which had Relapse |
# Sites with Cleft Severity >15 and ≤30 (n=11) which had Relapse |
# Sites with Cleft Severity >30 (n=4) which had Relapse |
Total # Relapse (n=61) |
|
|
Total |
7 (28%) |
10 (47.62%) |
6 (54.55%) |
2 (50%) |
25 (40.98%) |
|
Controls (n=19) |
3 |
2 |
2 |
0 |
7 |
|
Experimentals (n=42) |
4 |
8 |
4 |
2 |
18 |
Forty-six of the sites had previously measured severity values from the preceding investigation. 30 of these sites decreased in their gingival cleft severity while 16 increased in severity.
II Gingival Phenotype
Gingival thickness measurements were taken from the preceding investigation and used to place subjects in this study into two groups: Thin gingival phenotype (less than or equal to 2.5mm) and thick gingival phenotype (greater than 2.5mm). These measurements from the previous study were taken by transgingival probing on the buccal surface prior to tooth extraction. Because of the availability of these previous measurements, only 41 sites were compared instead of the total 61 in this study. Twenty-one sites were part of the thin gingival group and 9 (42.86%) showed relapse (Table 3). Of these 9, 6 (66.67%) entered the study with a cleft. 20 sites were part of the thick gingival group with 9 (45%) having relapse. Of these 9, 7 (77.78%) came into the study with a cleft. A graphical representation of thin vs. thick gingival phenotype and the incidence of relapse associated with each is show in (Graph 1).
Table 3: Gingival Phenotype Data.
|
Gingival Phenotype with Relapse |
|||
|
Thin Relapse # (n=21) |
Thick Relapse #(n=20) |
Total# Relapse (n=41) |
|
|
|
|
|
|
|
Total |
9 (42.86%) |
9 (45%) |
18 (43.90%) |
|
Controls (n=19) |
3 |
2 |
5 |
|
Experimentals (n=42) |
6 |
7 |
13 |
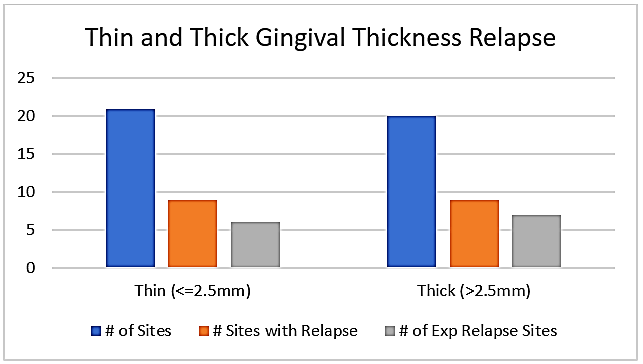
Graph 1: Thin and Thick Gingival Thickness Relapse.
Of those sites in the thin gingival group the mean cleft severity was 7.63 mm2, and of those sites in the thick gingival group the mean cleft severity was 12.00 mm2.
Discussion
There were no statistically significant correlations found when comparing the incidence of relapse with the presence of a gingival cleft, or distance of relapse with the presence of a gingival cleft. When comparing the control and experimental groups to incidences of relapse, 36.84% and 42.86% respectively, as well as to the distance of relapse, no statistically significant (p<0.05) correlations were found. Hence, this investigation could have benefited from an equal number of control and experimental sites. From the available subjects and sites this was not possible to measure an equal amount of control sites.
I Severity
Of the sites which did relapse, a greater relapse distance occurred in sites with increased cleft severity. A significant positive correlation between cleft severity and the distance of relapse (p<0.05) was determined. However, no statistically significant correlation was found when comparing cleft severity and the incidence of relapse. From this data one can infer that whether a cleft has a high severity or low severity does not predilect the site for having relapse vs. no relapse at all. As the gingival cleft severity between adjacent teeth increases, the defect area (i.e. the lack of bone, soft tissue, or both) must increase as well. Previous investigations were able to determine that gingival invaginations could very well persist for up to 5 years after completion of orthodontic treatment [7]. If, in fact, gingival invaginations persist for this amount of time it would be reasonable to assume this is why not more sites in this study decreased in severity value.
II Relapse
Circuns (1983) analyzed the relationship between reopening of extraction spaces and gingival clefts [7]. In that study of 72 patients no correlations were established regarding space reopening between those in retention wearing retainers for at least 6 months and those who had completed retention (average of 29 months) and not worn retainers for at least 6 months [7]. There was no consistent relationship found when looking at the amount of space reopening with the presence and severity of gingival invaginations [4]. The primary goal of orthodontics is the precise alignment of teeth and the establishment of a stable occlusion, yet if there is a possibility of reopening a space to a distance of 0.128mm (which was the average relapse distance in our study), is surgical treatment deemed necessary to excise the invagination and would this be worth an invasive procedure to the patient? In the literature a study evaluated the effect of orthodontic retention on the mechanical properties of the periodontal ligament using rat maxillary first and second molars. It was found that during the application of orthodontic forces the elastic stiffness of the periodontal ligament decreased greatly [16].
However, the elastic stiffness of the PDL increased gradually and reached control levels eight days after retention. Thus, when measuring the amount of reopened space on the day of orthodontic appliance removal, it could give way to greater initial measurements since the PDL elastic stiffness may be weakened permitting a larger IPR thickness gauge to fit interproximal. Another study observed the presence of inflammation in periodontal tissues after introduction of orthodontic forces [17]. They stated that inflammatory reactions in the periodontium are produced from orthodontic forces and that levels of inflammatory mediators in gingival crevicular fluid have been shown to be elevated during orthodontic treatment. With noticeable capillary vasodilation in the PDL during orthodontic force exertion comes the migration of inflammatory cells and cytokine production [18]. These findings could lead to greater initial measurements at the time of fixed appliance removal, thus may not be a true representation of the amount of relapse determined.
III Gingival Phenotype
When comparing the thin and thick gingival phenotype groups, 42.86% and 45% relapsed respectively. Even though the sites with a thick gingival phenotype had a higher percentage of relapse, this wasn’t statistically significant in our study. When comparing gingival phenotype thickness with relapse and gingival phenotype thickness with gingival cleft severity, no statistically significant correlations were found.
Stappert (2018) found a negative association between gingival thickness and cleft severity, and there was no association exhibited between cleft severity and keratinized gingiva [14]. The sites with thinner gingival thickness exhibited a greater tendency for development of gingival clefts in terms of severity and occurrence than those with a thick gingival thickness. In this current study, however, the sites with a thinner gingival thickness exhibited a smaller mean cleft severity than those sites with a thick gingival thickness (though not found to be statistically significant). Considering the number of experimental sites in this current study was twice that of the control sites, an additional piece of data which stood out is that 3.5 times more experimental sites showed relapse with a thick gingival phenotype compared to the control sites.
From this information we can extrapolate clinical usefulness and relate it to patient care. For instance, if a clinician notices the formation of a gingival cleft during orthodontic treatment with a thick gingival phenotype, the clinician can caution the patient about the increased likelihood of post-treatment relapse in that area. The clinician could provide ways to reduce this outcome such as explaining gingival excision procedures, thus not surprising the patient if in fact they have relapse in the future.
IV Retention
When considering the findings related to gingival clefts and relapse, as well as gingival cleft severity, it is incumbent upon the orthodontist to determine if the presence of the gingival cleft is clinically acceptable. Would removing a gingival cleft toward the end of orthodontic treatment (just prior to debond) really affect the patient? Edwards in 1971 discussed retention and gingival tissue, stating, “it would not be advisable or practical, from a periodontal point of view, to remove an excessive amount of attached gingiva or to eliminate the interdental papilla completely” [5]. If inflammation assists in the destruction of the disorganized gingival fibers while newly formed fibers align in a more compatible way with orthodontically treated teeth to lessen relapse, maybe gingival injection of the collagenase enzyme should be considered [7].
The author also mentioned that gingival invaginations could persist for up to 5 years after completion of orthodontic treatment [7]. If this holds true it should be considered practical to continue fixed retention and retainer wear up to this 5-year mark. Future studies could examine subjects for an even longer period of time (5 years or more) evaluating the long-term presence of gingival clefts and if prolonged persistence has effects on orthodontic relapse. A systematic review of orthodontic retention evaluated the efficacy of retention strategies [19]. They found a statistically significant increase in stability in both the mandibular and maxillary segments when circumferential supracrestal fiberotomies were performed in conjunction with wearing a Hawley retainer versus wearing a Hawley alone. However, they concluded that there is insufficient evidence on which to base the clinical practice of orthodontic retention.
In this study the method of retention among subjects varied considerably. Some were given clear Essix retainers, Hawleys (different variations fabricated among patients) or lingual fixed retainers, and due to these different appliances, the variable of retention was not included in this study. Moreover, it was not possible to control for patient compliance with regards to wearing retainers on a defined regimen. It was found that whether a patient wears or does not wear a retainer plays a large role in whether there is relapse after orthodontic treatment, and that there is a noticeable decrease in compliance with regards to retainer wear as time elapses from the date of fixed appliance removal [20].
V Limitations
Some subjects who were part of the preceding investigation were still in orthodontic treatment when the measurements for this study were being made, thus the number of subjects decreased from the available 42 to 18. 2 subjects who were enrolled in this study only came in one time for measurements at their debond appointment day and considering we could not follow them throughout an extended period of months into retention to record any changes observed, their measurements were not incorporated into the statistical analysis. The measurement protocol (5 time points) was not realized for all patients, because they rescheduled and cancelled retention appointments frequently. Inter-rater reliability as well as setting a standard for recording measurements was not able to be determined for this study as there were different recorders in the preceding investigation from this one.
Summary and Conclusions
As cleft severity increases, the amount of relapse distance of extraction areas is likely to increase as well. In patients with a thick gingival phenotype who obtain gingival clefts in extraction sites during orthodontic treatment, it is more likely that these sites will have dental relapse post-treatment compared to sites which did not develop a gingival cleft. It is incumbent upon the clinician to use sound judgement whether or not to consider the necessity to excise gingiva in extraction spaces to prevent space reopening. Because gingival clefts have been shown to persist for many years, strict retention protocols should be utilized to decrease even the possibility of relapse in these particular sites. Sites that are prone to relapse are thus prone to food impaction which can damage the periodontium and alter the otherwise stable occlusion which is a goal of orthodontic therapy.
APPENDIX A
Electronic digital caliper measurements of the width of the periodontal probe:
Hu-Friedy PCPMDBIU
Probe length (mm)
Probe width (mm)
0
0
0.5
0.46
1.0
0.49
1.5
0.51
2.0
0.53
2.5
0.56
3.0
0.59
3.5
0.60
4.0
0.61
4.5
0.64
5.0
0.68
5.5
0.70
6.0
0.71
6.5
0.74
7.0
0.76
7.5
0.78
8.0
0.81
8.5
0.83
9.0
0.85
9.5
0.88
10.0
0.91
Conflicts of Interest
None.
Funding
None.
Article Info
Article Type
Research ArticlePublication history
Received: Fri 17, Jan 2020Accepted: Thu 19, Mar 2020
Published: Tue 31, Mar 2020
Copyright
© 2023 Dina Stappert . This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.DOBCR.2020.01.05
Figures & Tables
Table 1: Control vs. Experimental Data.
|
Controls vs. Experimental |
||
|
# Controls (n=19) with Relapse |
# Experimental (n=42) with Relapse |
Total # (n=61) with Relapse |
|
7 (36.84%) |
18 (42.86%) |
25 (40.98%) |
The average reopening space was 0.128mm with a range of 1.8mm having a minimum of -0.3mm and maximum of 1.5mm. The relapse median and mode were both 0mm.
Table 2: Severity Data.
|
Cleft Severity (mm2) with Relapse |
|||||
|
# Sites with Cleft Severity of 0 (n=25) which had Relapse |
# Sites with Cleft Severity >0 and ≤15 (n=21) which had Relapse |
# Sites with Cleft Severity >15 and ≤30 (n=11) which had Relapse |
# Sites with Cleft Severity >30 (n=4) which had Relapse |
Total # Relapse (n=61) |
|
|
Total |
7 (28%) |
10 (47.62%) |
6 (54.55%) |
2 (50%) |
25 (40.98%) |
|
Controls (n=19) |
3 |
2 |
2 |
0 |
7 |
|
Experimentals (n=42) |
4 |
8 |
4 |
2 |
18 |
Forty-six of the sites had previously measured severity values from the preceding investigation. 30 of these sites decreased in their gingival cleft severity while 16 increased in severity.
Table 3: Gingival Phenotype Data.
|
Gingival Phenotype with Relapse |
|||
|
Thin Relapse # (n=21) |
Thick Relapse #(n=20) |
Total# Relapse (n=41) |
|
|
|
|
|
|
|
Total |
9 (42.86%) |
9 (45%) |
18 (43.90%) |
|
Controls (n=19) |
3 |
2 |
5 |
|
Experimentals (n=42) |
6 |
7 |
13 |
The type of retention appliance used by each subject was recorded.
References
- Dardengo CS, Fernandes LP, Capelli Júnior (2016) Frequency of orthodontic extraction. Dental Press Journal of Orthodontic. Dental Press J Orthod 21: 54-59. [Crossref]
- Gorbunkova A, Pagni G, Brizhak A, Farronato G, Rasperini G (2016) Impact of Orthodontic Treatment on Periodontal Tissues: A Narrative Review of Multidisciplinary Literature. Int J Dent 2016: 4723589. [Crossref]
- Golz L, Reichert C, Dirk C, Jager A (2012) Retrospective investigation of gingival invaginations: Part II: microbiological findings and genetic risk profile. J Orofac Orthop 73: 387-396. [Crossref]
- Wehrbein H, Bauer W, Deidrich PR (1995) Gingival invagination area after space closure: A histologic study. Am J Orthod Dentofac Orthop 108: 593-598. [Crossref]
- Edwards JG (1971) The prevention of relapse in extraction cases. Am J Orthod 60: 128-144. [Crossref]
- Reitan K (1959) Tissue rearrangement during detention of orthodontically rotated teeth. Angle Orthod 29: 105-113.
- Rivera Circuns AL, Tulloch JF (1983) Gingival invagination in extraction sites of orthodontic patients: their incidence, effects on periodontal health, and orthodontic treatment. Am J Orthod 83: 469-476. [Crossref]
- Reichert C, Kutschera E, Nienkemper M, Scharf S, Mengel M et al. (2013) Influence of time after extraction on the development of gingival invagination: study protocol for a multicenter pilot randomized controlled clinical trial. Trials 14: 108. [Crossref]
- Kurol J, Ronnerman A, Heyden G (1982) Long-term gingival conditions after orthodontic closure of extraction sites. Histological and histochemical studies. Eur J Orthod 4: 87-92. [Crossref]
- Atherton JD (1970) The gingival response to orthodontic tooth movement. Am J Orthod 58: 179-186. [Crossref]
- Parker GR (1972) Transeptal fibers and relapse following bodily retraction of teeth: a histologic study. Am J Orthod 61: 331-344. [Crossref]
- Malkoc S, Bayukyllmaz T, Gelgor I, Gursel M (2004) Comparison of two different gingivectomy techniques for gingival cleft treatment. Angle Orthod 74: 375-380. [Crossref]
- Thompson HE (1959) Orthodontic relapses analyzed in a study of connective tissue fibers. Am J Orthod 45: 93-109.
- Stappert D, Geiman R, Heidari ZH, Reynolds MA (2018) Gingival clefts revisited: Evaluation of the characteristics that make one more susceptible to gingival clefts. Am J Orthod Dentofacial Orthop 145: 677-682. [Crossref]
- Reichert C, Wenghöfer M, Götz W, Jäger A (2011) Pilot study on orthodontic space closure after guided bone regeneration. J Orofac Orthop 72: 45-50. [Crossref]
- Hong RK, Yamane A, Kuwahara Y, Chiba M (1992) The effect of orthodontic retention on the mechanical properties of the periodontal ligament in the rat maxillary first molar. J Dent Res 71: 1350-1354. [Crossref]
- Yamaguchi M, Kasai K (2005) Inflammation in periodontal tissues in response to mechanical forces. Arch Immunol Ther Exp 53: 388-398. [Crossref]
- Meeran NA (2013) Cellular response within the periodontal ligament on application of orthodontic forces. J Indian Soc Periodontol 17: 16-20. [Crossref]
- Littlewood SJ, Millett DT, Doubleday B, Bearn DR, Worthington HV (2006) Orthodontic Retention: A Systematic Review. J Orthod 33: 205-212. [Crossref]
- Pratt MC, Kluemper GT, Lindstrom AF (2011) Patient Compliance with Orthodontic Retainers in the Postretention Phase. Am J Orthod Dentofacial Orthop 140: 196-201. [Crossref]