Prominent Eustachian Valve Mimicking Thrombus in Right Atrium Diagnosed with Computed Tomography in a Patient with Atrial Fibrillation
A B S T R A C T
A 51-year-old man presented with paroxsysmal atrial fibrillation (AF). Transthoracic echocardiography revealed mass of 2.3x0.6 cm adjacent to the superior part of the right atrium (RA) compatible with thrombus. Although thrombus formation in the setting of AF is more common in left atrial appendage and left atrium it can also be seen in right atrial appendage and RA. We performed cardiac computerized tomography (CCT) in order to clarify the nature of mass in RA and exclude coronary stenosis. CCT showed prominent eustachian valve measuring 3.2 cm which was not clear on echocardiography. This case underscores the importance of complementary cardiovascular imaging to facilitate the correct diagnosis.
Keywords
Atrial fibrillation, thrombus, transthoracic echocardiography, cardiac computerized tomography
Case Presentation
A 51-year-old man with no previously known disease was admitted to our clinic with palpitation, atypical chest pain and syncope. He had a family history of coronary artery disease (father had myocardial infarction at the age of 52) and smoking risk factor. On admission, his blood pressure was 110/60 mmHg, heart rate was irregular and 140/min. Electrocardiogram revealed rapid ventricular rate atrial fibrillation (AF) which returned to normal sinus rhythm after 5 mg intravenous metoprolol. Transthoracic echocardiography showed normal ejection fraction (60%), mild mitral and tricuspid regurgitation and mildly dilated left atrium (43 mm in parasternal long axis view, 23 cm2 in apical 4 chamber view). There was an hyperechogenic, oval shaped mass measuring 2.3x0.6 cm adjacent to the superior part of the right atrium (Figure 1). As the patient had paroxysmal AF, risk factors for coronary artery disease and had atypical chest pain, we decided to exclude a likely thrombus in the right atrium and simultaneous coronary artery disease, hence we performed a cardiac CT (CCT). CCT showed a prominent eustachian valve measuring 3.2 cm which was not clear on echocardiography (Figure 2). There was neither mass in the right atrium nor significant coronary artery disease and we were able to exclude 2 possible pathologies with a single, simple imaging modality.
Discussion
Since AF is associated with an increased risk of atrial thrombus formation and embolism, we thought that the mass we appreciated in the right atrium might be thrombus. Although thrombus formation in the setting of AF is more common in left atrial appendage and left atrium it can also be seen in the right atrial appendage and right atrium [1-2]. Transeoshopageal echocardiography is the most commonly used method to search for the thrombus. In the era of cardiac multimodality imaging, we can use tailored imaging modalities like CCT and cardiac magnetic rezonanse to provide multiple information.
It is extremely crucial to be able to utilize complementary cardiovascular imaging modalities in different patient groups to facilitate the diagnosis. It improves cost effectivity, by decreasing the number of diagnostic tests and gives quicker result which is necessary to decide on the definitive treatment.
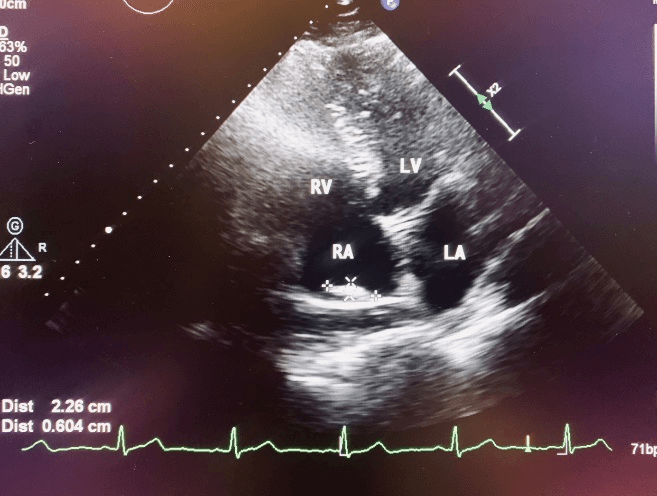
Figure 1: Transthoracic echocardiography apical 4 chamber view demonstrating right atrial mass adjacent to superior wall of the right atrium. RV: right ventricle, RA: right artium, LV: left ventricle, LA: left atrium.
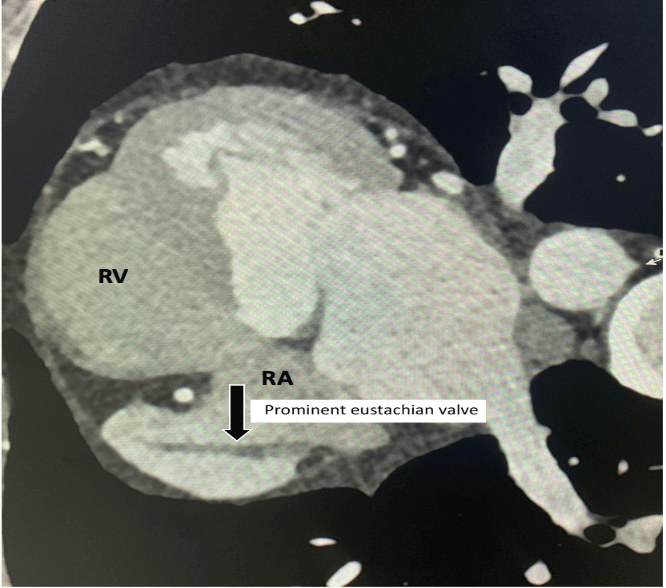
Figure 2: Cardiac computed tomography axial view demonstrating prominent eustachian valve in the right atrium. RV: right ventricle, RA: right artium.
Article Info
Article Type
Case ReportPublication history
Received: Mon 20, Apr 2020Accepted: Wed 27, May 2020
Published: Mon 08, Jun 2020
Copyright
© 2023 Ibrahim SARI. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.RDI.2020.02.02
Figures & Tables
References
- V Rozenberg, F Boccara, B Benhalima, N Lamisse, B Buyukoglu et al. (2000) Comparison of echocardiographic markers of embolism in atrial flutter and fibrillation: frequency of protruding atherosclerotic plaques in the thoracic aorta. Echocardiography 17: 555-562. [Crossref]
- Orhan Ozer, Ibrahim Sari, Vedat Davutoglu (2010) Right atrial appendage: forgotten part of the heart in atrial fibrillation. Clin Appl Thromb Hemost 16: 218-220. [Crossref]