Mucoepidermoid Carcinoma: Unusual Localisation
A B S T R A C T
Introduction: Mucoepidermoid carcinoma (MEC) is a rare malignant tumor that develops from the salivary glands. Its treatment includes surgery associated or not with radiotherapy depending on the histological grade. We report the case of a 38-year-old patient.
Methods: We report a case of a mucoepidermoid carcinoma of the palate, and we specify the clinical, therapeutic and progressive characteristics of this attack.
Case Report: She is a 38-year-old woman with no significant medical history. The clinical examination revealed a localized mass at the level of the hard palate, with a smooth normal-looking mucosa measuring 4 cm in long axis, the rest of the clinical examination was normal. Pathology examination confirmed the diagnosis of low-grade CME. Magnetic resonance imaging was performed objectifying a lesion localized at the level of the submucosa of the palate without bone extension either to the tongue or to the nasal cavity. The treatment consisted in excision of the lesion with margin, with monthly monitoring for 6 months with good progress.
Conclusion: The discovery of a CME in young patients is rare. This observation makes it possible to take stock of the management of this type of cancer according to histological characteristics.
Keywords
Mucoepidermoid, palate, minor salivary gland
Introduction
Mucoepidermoid carcinoma (MEC) is an epithelial salivary gland neoplasm. About 5% of these occur in younger age group usually less than 18 years with female predominance [1, 2]. It is composed of mucus, squamous, and intermediate type of cells [3]. About two-third of MEC arise within the parotid gland, and one-third develops within the minor salivary glands. When it develops in minor salivary glands, it can be located on the palate, retromolar area, floor of the mouth, buccal mucosa, lips, and tongue. It most frequently occurs in the fifth and sixth decades of life [3].
Case Report
A 38-year-old woman with no significant medical history. Reporting the appearance of a swelling in the level of the hard palate. Intraoral examination revealed a localized mass at the level of the hard palate, with a smooth normal-looking mucosa measuring 4cm in long axis, the rest of the clinical examination was normal. No toothache, pain, altered taste, sensation, numbness, pus discharge, bleeding from nose, trauma, extraction or weight loss (Figure 1).
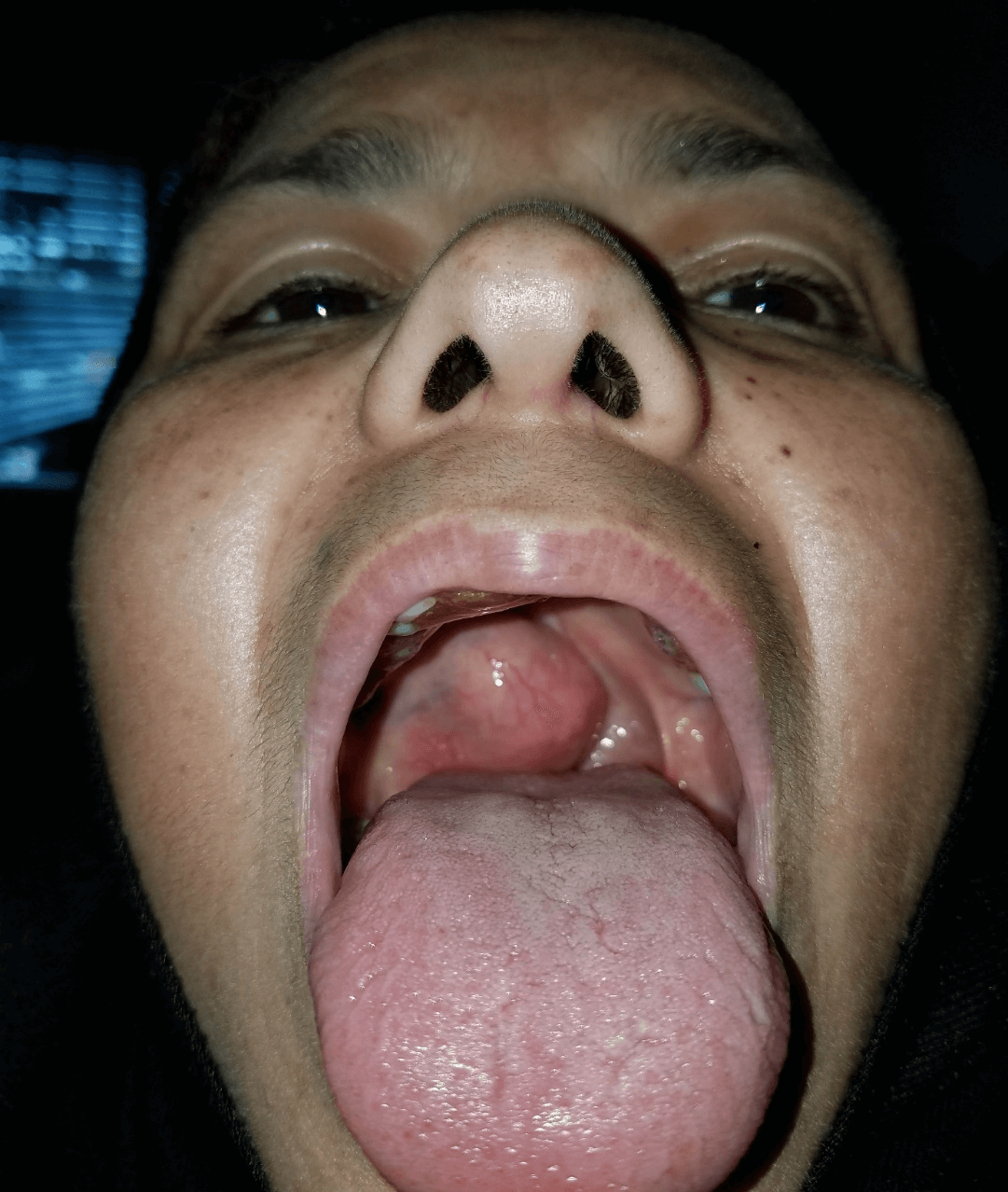
Figure 1: Macroscopic aspect of the mass.
Incisional biopsy was done pathology examination confirmed the diagnosis of low-grade CME. Magnetic resonance imaging was performed objectifying a lesion localized at the level of the submucosa of the palate without bone extension either to the tongue or to the nasal cavity (Figure 2).
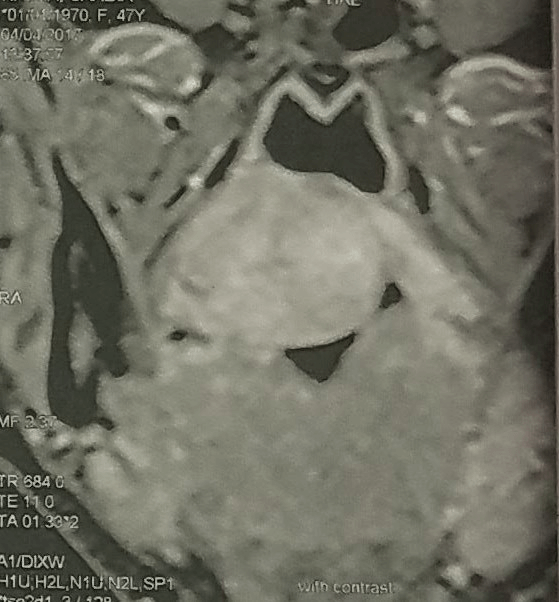
Figure 2: Facial magnetic resonance imaging showing a regular mass of the submucosa of the palate.
The treatment consisted in excision of the lesion with margin, with monthly monitoring for 6 months with good progress. On histopathology examination, H and E staining showed three groups of cells, namely large mucous cells with an empty cytoplasm and peripherally placed nucleus, intermediate cells with basaloid nucleus, and epidermoid cells with eosinophilic cytoplasm suggestive of intermediate-grade MEC, following which a wide surgical excision with adjacent free margins was carried out. Postoperative healing was uneventful. Patient was followed up for a year and no recurrence reported (Figure 3).
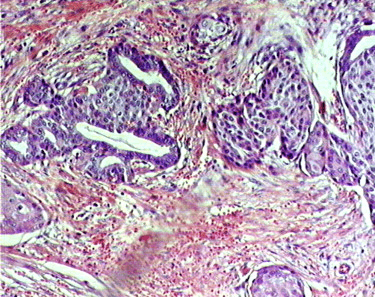
Figure 3: Microscopic aspect of the histopathological examination showing characteristics of MEC.
Discussion
It accounts for <3% of all head and neck tumors with a female predilection [4, 5]. It occurs commonly in parotid glands and minor salivary gland is the second most common site. Clinically, the majority of palatal MEC appears as firm, painless swellings, it mimic mucoceles or vascular lesions. The percentage of benign tumors occurring in the palate is higher than that of malignant tumors [6, 7]. Histologically, mucoepidermoid carcinoma have been categorized into one of three histopathologically based on the amount of cyst formation, degree of cytologic atypia, relative numbers of mucous, epidermoid and intermediate cells [8].
In the low-grade tumors show prominent cyst formation, minimal cellular atypia and high proportion of mucous cells, in opposition High-grade tumors consist of solid islands of epidermoid and intermediate cells. They also demonstrate considerable pleomorphism and mitotic activity. Mucous producing cells infrequent, difficult to distinguish from squamous cell carcinoma. [9, 10] Low to intermediate-grade MECs originating from intraoral minor salivary glands can be managed by wide local surgical excision that ensures tumor-free surgical margins according to Moraes et al. [9-11].
If there is no evidence of bony involvement the tumor should be dissected down to the periosteum. If there is any evidence of periosteal involvement or bone erosion, removal of the involving bone is indicated. High-grade tumors require more aggressive surgical approach with postoperative radiotherapy and chemotherapy. Low- to intermediate-grade MECs originating from intraoral minor salivary glands has a very low recurrence rate (<10%) and a high survival rate (90%). 10 Low and intermediate grade MECs have an indolent clinical course and a rare chance for metastasis. Radical neck dissection is indicated if clinical evidence of metastasis. Prognosis depends on grade and stage of tumor [10, 11]. Low and intermediate grade MEC in this age group can recur many years later, so a close clinical follow-up should be for lifetime.
Conclusion
The discovery of a MEC in young patients is rare. This observation makes it possible to take stock of the management of this type of cancer according to histological characteristics. Low grade may be treated with surgical excision only with a lifetime follow-up because of late recurrence possibility.
Article Info
Article Type
Case ReportPublication history
Received: Thu 27, Feb 2020Accepted: Thu 19, Mar 2020
Published: Mon 30, Mar 2020
Copyright
© 2023 Zouhair Najib. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.CMCR.2020.01.03
Figures & Tables
References
- Hicks J, Flaitz C (2000) Mucoepidermoid carcinoma of salivary glands in children and adolescents: assessment of proliferation markers. Oral Oncol 36: 454-460. [Crossref]
- Luna MA, Batsakis JG, el Naggar AK (1991) Salivary gland tumors in children. Ann Otol Rhinol Laryngol 100: 869-871. [Crossref]
- Neville BW, Damm D, Allen CM, Bouquot JE (2009) Salivary gland pathology. Oral and Maxillofacial Pathol 495-497.
- da Cruz Perez DE, Pires FR, Lopes MA, de Almeida OP, Kowalski LP (2006) Adenoid cystic carcinoma and mucoepidermoid carcinoma of the maxillary sinus: report of a 44-year experience of 25 cases from a single institution. J Oral Maxillofac Surg 64: 1592-1597. [Crossref]
- Flaitz CM (2000) Mucoepidermoid carcinoma of the palate in a child. Pediatr Dent 22: 292-293. [Crossref]
- Rajendran R (2009) Tumors of the salivary gland. In: Rajendran R, Sivapathasundharam B, editors, ed. Shafer’s Textbook of Oral Pathology. India: Elsevier 219-253.
- Moshy J, Owibomaingere S, Mwakyoma H (2010) Intraoral minor salivary glands neoplasms; the pattern and management. Prof Med J 17: 483-489.
- Munhoz Ede A, Cardoso CL, Tjioe KC, Sant'ana E, Consolaro A et al. (2009) Atypical clinical manifestation of mucoepidermoid carcinoma in the palate. Gen Dent 57: e51-e53. [Crossref]
- Moraes P, Pereira C, Almeida O, Perez D, Correa ME et al. (2007) Paediatric intraoral mucoepidermoid carcinoma mimicking a bone lesion. Int J Paediatr Dent 17: 151-154. [Crossref]
- April MM, Brodsky LS, Cunningham MJ, Harari PM, Harrison L et al. (1997) Mucoepidermoid carcinoma in a 10-year-old girl. Head Neck 19: 431-435. [Crossref]
- Ritwik P, Cordell KG, Brannon RB (2012) Minor salivary gland mucoepidermoid carcinoma in children and adolescents: a case series and review of the literature. J Med Case Rep 6: 182. [Crossref]