Journals
Mesiodens Diagnosis and Management: Series of Case Report
A B S T R A C T
Mesiodens are the most common supernumerary teeth, occurring in 0.15% to 1.9% of the population. Since its quite common, the general dentist should be aware about the signs and symptoms of mesiodens and its essential treatment. Mesiodens can cause delayed or ectopic eruption of the permanent incisors, which can further alter occlusion and esthetics. It is therefore important for the clinician to diagnose a mesiodens as early as possible to allow for optimal yet minimal treatment. Treatment options may include surgical extraction of the mesiodens.
K E Y W O R D S
Anomalies, Phylogenetic, dichotomy
I N T R O D U C T I O N
Developmental dental anomalies generally manifest as a variation in tooth size, shape, number, or structure. Supernumerary teeth are considered as one of the most significant dental anomalies during the primary and early mixed dentition. The prevalence of supernumerary teeth ranges from 0.10% to 3.9% in permanent dentition and 0.02% to 1.9% in primary dentition [1, 2]. Supernumerary teeth are encountered more frequently in males than in females in a ratio of 2:1 [2-5]. The exact etiology is not clearly understood. The literature reports 3 theories concerning the cause of mesiodens but it still remains controversial [6]. It was originally postulated that mesiodens represented a phylogenetic relic of extinct ancestors who had 3 central incisors [7]. This theory, known as phylogenetic reversion (atavism), has now been largely discarded by embryologists. A second theory known as dichotomy suggests that the tooth bud is split to create 2 teeth, one of which is the mesiodens [8]. Supporters of this theory believe that dichotomy represents complete germination, which also occurs frequently in the anterior maxilla. The third theory, involving hyperactivity of the dental lamina, is the most widely supported [6]. According to this theory, remnants the dental lamina or palatal offshoots of active dental lamina are induced to develop into an extra tooth bud, which results in a supernumerary tooth. Genetics are also thought to contribute to the development. Autosomal dominant inheritance with incomplete penetration has been the proposed genetic theory [8].
Supernumerary teeth are classified on the basis of position and form [9, 10]. Positional variations include mesiodens, paramolars, distomolars, or parapremolars and variations in the form consist of rudimentary and supplemental teeth. A rudimentary tooth may be conical, tuberculate, or molariform while a supplemental tooth is a supernumerary tooth which resembles the shape and size of the tooth it is associated with.
Mesiodens is a supernumerary tooth present between the maxillary central incisors. It is the most common type of supernumerary tooth with a prevalence of 0.15–2.2% [2, 5, 6, 11]. Mesiodens can occur individually or as multiples (mesiodentes), unilaterally or bilaterally, erupted or unerupted, in one or both jaws [11]. The presence of two mesiodens can significantly affect both occlusion and appearance by altering the eruption path and the position of the permanent incisors [2, 6, 7]. Multiple supernumerary teeth are frequently associated with various craniofacial anomalies including cleft lip and palate, Gardner’s syndrome, and cleidocranial dysostosis [12].
Clinical and Radiographic Diagnosis
A mesiodens should be suspected when there is asymmetry in the eruption pattern of the maxillary incisors; the maxillary primary incisors are overretained, especially if the over-retention is asymmetric; or there is significant ectopic eruption of one or both permanent maxillary incisors [6, 7, 13]. Given that only 25% of supernumerary teeth erupt, it is important to have a high index of suspicion in these situations.
Panoramic maxillary, occlusal, and periapical radiographs are essential in the diagnosis of impacted mesiodens. A panoramic radiograph serves as a screening aid and provides additional information about the associated supernumerary or congenitally missing teeth that are frequently seen with mesiodentes, but this type of imaging often yields limited evidence of the mesiodens itself because of lack of clarity in the midline region. The most accurate diagnostic radiographic method, to determine the bucco-lingual position of an unerupted supernumerary is by obtaining two periapical or maxillary occlusal radiographs which are analyzed according to the radiographic parallax principle [7, 14]. The identification of the path of eruption (normal, inverted, or horizontal) and the location (palatal or labial, superior or inferior) of the impacted mesiodens, relative to adjacent structures, help to formulate an appropriate treatment plan [2].
Case Report 1
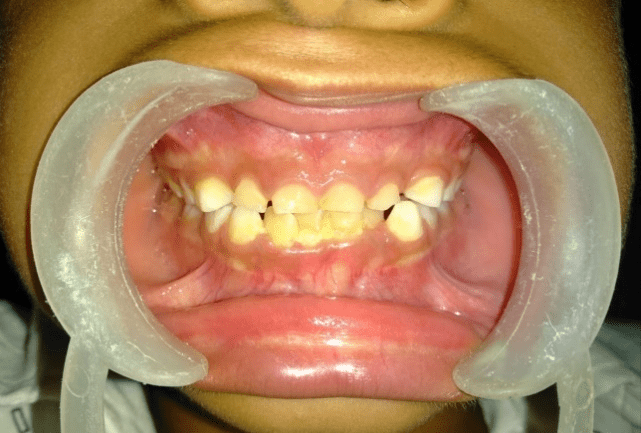
An 8-year-old boy was brought by his parents to the Dept. of Pedodontics, PGIDS, Rohtak. Their chief complaint was the non-eruption of the upper permanent central incisor. The child had no history of medical and dental trauma. The patient had a skeletal class I malocclusion and balanced facial pattern. Intraoral examination revealed an early mixed dentition and an Angle’s class I molar relationship. Clinical examination showed over retained central incisor (Figure 1) and no apparent arch length discrepancy in both maxillary and mandibular arches. Computed cone beam tomography of upper anterior region demonstrated a supernumerary tooth and an impacted permanent left central incisor (Figure 2).

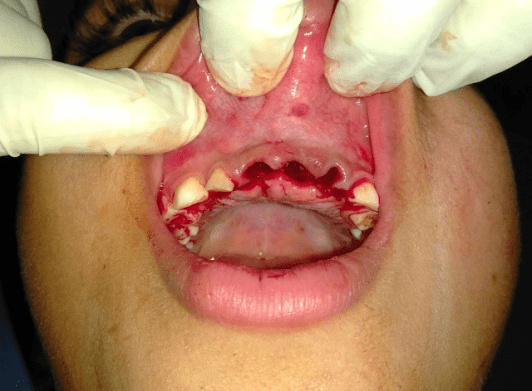
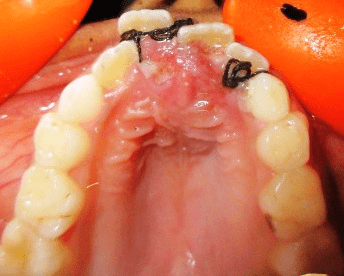
The treatment was carried out under local anesthesia, which involved extraction of primary incisors. The extraction was followed by raising the palatal flap and surgical extraction of palatally placed horizontally impacted mesiodens with dilacerated root (Figure 3). Sutures were given (Figure 4) and the patient was recalled after 1 week for suture removal. The patient is being followed at regular intervals to monitor the eruption of permanent central incisor.

Case Report 2
A 9-year-old girl reported to the Department of Pedodontics, PGIDS, Rohtak, with a complaint of extra teeth on palatal side. There was no history of trauma and her medical history was irrelevant. On clinical examination, late mixed dentition with malaligned central incisor were seen (Figure 1). There was a firm bulge palpable in the upper left central incisor area. On examining the radiographs, a dense opaque mass was seen in the left central incisor area, which was provisionally diagnosed as an odontome/supernumerary tooth.

An exploratory surgery was planned under local anaesthesia. On surgical exposure, a conical supernumerary tooth was found palatal to the left central incisor. Both erupted and impacted supernumerary tooth were extracted and the flap was closed. Since child is in ugly duckling stage so for a while fixed orthodontic treatment is kept on halt and if required will be planned after age of 12 to correct the residual malalignment.


Case Report 3
A 10-year age boy reported to the the Department of Pedodontics, PGIDS, Rohtak, with a complaint of palpable bulge on palate. On clinical examination, late mixed dentition with malaligned central incisor were seen (Figure 1). There was a firm bulge palpable in the midline area. On examining the radiographs, a dense opaque mass was seen in right central incisor area, which was provisionally diagnosed as an odontome/supernumerary tooth. A surgical exploratory process was carried under local anaesthesia and mesiodense was surgically removed so as to avoid complications which could have arrived due to supernumerary teeth.
An exploratory surgery was planned under local anaesthesia. On surgical exposure, a conical supernumerary tooth was found palatal to the left central incisor. Both erupted and impacted supernumerary tooth were extracted and the flap was closed. Since child is in ugly duckling stage so for a while fixed orthodontic treatment is kept on halt and if required will be planned after age of 12 to correct the residual malalignment.




Discussion
The presence of an extra tooth has great potential to disrupt normal occlusal development and hence esthetics of child. The presence, position, and relation of super numerary teeth to the adjacent teeth, and distance of the impacted permanent tooth from occlusal plane should be evaluated on the radiographic basis. An early recognition of the supernumerary teeth is essential for determining the appropriate treatment for each patient.
In Case 1, impaction of maxillary permanent left central incisor due the presence of one supernumerary tooth placed left to the midline was observed in the male child who was in the mixed dentition stage with no associated craniofacial syndrome. Ersin et al1 reported mesiodens to be more in males (i.e., in the ratio of 3:1), mean age for the diagnosis of mesiodens was 8.96 years and were more frequently located on the left side of the midline (and none at the midline). In this case, surgical treatment was performed to extract the supernumerary tooth lying incisal to the impacted permanent upper central incisor to bring the unerupted maxillary incisor into proper alignment. Reports say that a majority of the unerupted teeth (approximately 75%) will erupt once the supernumerary tooth is removed.
In Case 2, the supernumerary tooth was two mesiodens. The most common complication of mesiodens is displacement of central incisors [15]. The treatment was aimed at extraction of mesiodens with no orthodontic treatment for alignment of permanent central incisor as patient is in ugly duckling stage.
In Case 3, the supernumerary teeth present on palatal aspect was extracted as soon as diagnosed to prevent complications like resorption of roots of adjacent teeth, root anomaly, cyst formation, and intra-oral infection [5, 14, 16].
The timing of surgical removal of supernumerary teeth is contentious and two alternatives exist. First, to remove the supernumerary as soon as it has been diagnosed and second, to leave the supernumerary as such till the root development of adjacent teeth is complete in order to prevent damage to their root apices [4]. However, no evidence of root resorption, loss of vitality, or any disturbance to root development has been reported by Hogstrom and Andersson [4].
In all the present cases, surgical extraction of supernumerary teeth was done as soon as it was diagnosed, without any damage to adjacent teeth. The patients are being monitored at regular intervals.
Conclusion
The position, location, and type of supernumerary tooth and the level of co-operation of the child influence the treatment plan. However, each case should be assessed accordingly.
An early diagnosis and timely intervention could either prevent serious complications or limit the need for orthodontic treatment.
Article Info
Article Type
Research ArticlePublication history
Received 20 September, 2018Accepted 8 October, 2018
Published 16 November, 2018
Copyright
© 2018 Monika Rohilla. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository. All rights reserved.10.31487/j.ORD.2018.01.001
Author Info
Corresponding author
Monika RohillaDepartment of Paedodontics and Preventive Dentistry, Post Graduate Institute of Dental Sciences, Rohtak, India
Figures & Tables
References
1. Ersin NK, Candan U, Alpoz AR, Akay C (2004) Mesiodens in primary, mixed and permanent dentitions—a clinical and radiographic study. J Clin Pediatr Dent 28: 295-298. [Crossref]
2. Russell KA, Folwarczna MA (2003) Mesiodens—diagnosis and management of a common supernumerary tooth. J Can Dent Assoc 69: 362-366. [Crossref]
3. Ramsaran AS, Barclay S, Scipio E, Ogunsalu C (2005) Non-syndromal multiple buried supernumerary teeth: report of two cases from the English-speaking Caribbean and a review of the literature. West Indian Med J 54: 334-336. [Crossref]
4. Hogstrom A, Andersson L (1987) Complications related to surgical removal of anterio supernumerary teeth in children. ASDC J Dent Child 54: 341-343. [Crossref]
5. Gündüz K, Celenk P, Zengin Z, Sümer P (2008) Mesiodens—a radiographic study in children. J Oral Sci 50: 287-291. [Crossref]
6. Primosch RE (1981) Anterior supernumerary teeth — assessment and surgical intervention in children. Pediatr Dent 3: 204-215. [Crossref]
7. von Arx T (1992) Anterior maxillary supernumerary teeth: a clinical and radiographic study. Aust Dent J 37: 189-195. [Crossref]
8. Sedano HO, Gorlin RJ (1969) Familial occurrence of mesiodens. Oral Surg Oral Med Oral Pathol 27: 360-361. [Crossref]
9. Mitchell L (1989) Supernumerary teeth. Dent Update 16: 65-69. [Crossref]
10. Garvey MT, Barry HJ, Blake M (1999) Supernumerary teeth—an overview of classification, diagnosis and management. J Can Dent Assoc 65: 612-616. [Crossref]
11. Asaumi JI, Shibata Y, Yanagi Y, Hisatomi M, Matsuzaki H, et al. (2004) Radiographic examination of mesiodens and their associated complications. Dento Maxillo Facial Radiol 33: 125-127. [Crossref]
12. Gorlin RJ, Cohen MM, Hennekam RC (2001) In: Syndromes of the Head and Neck 4th ed. New York: Oxford University Press.
13. Konchak PA, Lanigan DT (1985) The management of impacted maxillary incisors secondary to supernumeraries. Oral Health 75: 59-61.
[Crossref]
14.Goaz SW (1987). In: Radiology Principles and Interpretation. St. Louis: Mosby Company.
15. Hattab FN, Yassin OM, Rawashdeh MA (1994) Supernumerary teeth: Report of three cases and review of the literature. ASDC J Dent Child 61: 382-393. [Crossref]
16. Kim SG, Lee SH (2003) Mesiodens: a clinical and radiographic study. J Dent Child (Chic) 70: 58-60. [Crossref]