Management of Enteroatmospheric Fistula and Floating Ileostomy: Would Eaken Wound Pouch Be the Answer? A Case Report
A B S T R A C T
Enterocutaneous and enteroatmospheric fistulas are the most challenging complications of abdominal sepsis to deal with a high mortality. This is even more challenging with a stoma in an open abdomen. In the setting of chronic granulomatous inflammation like abdominal tuberculosis or inflammatory bowel disease, recovery is prolonged and management involves multidisciplinary care. We present a rare case that was a complication of tuberculous peritonitis.
Keywords
Enteroatmospheric fistula, enterocutaneous fistula, floating stoma, tuberculous peritonitis
Introduction
Enteroatmospheric fistula is the occurrence of a fistula in an open abdomen. It has no tract and is not supported by granulation tissue. A floating stoma is a stoma in an open abdomen also not surrounded by skin or granulation tissue. In combination with a stoma in an open abdomen, this fistula presents a challenging problem for the surgeon due to the following reasons [1, 2].
i. The wound is difficult to resolve due to the repetitive exposure to the continuous non controlled exuding intestinal fluid from the stoma.
ii. Efforts to control the drainage from a fistula or stoma within the open abdomen may prove significantly more challenging than those used in the management of enterocutaneous varieties [3].
iii. Commonly surrounded by an adhered mass of granulating bowel without an appropriate surface amenable to appliance placement, even the initial diversion of drainage from the wound is a substantial problem [4, 5].
iv. The economic impact of fistula management is staggering, with prolonged hospital stay and increased morbidity and mortality.
Although management of floating stoma or enteroatmospheric fistula still evolving as there is no standard therapy, still principles of skin protection, fluid and nutritional support and control of infection apply [6]. Here, we present a solution which might be the way out of this difficult situation.
Case Presentation
A 32-year-old man was referred from Mandera County Teaching and Referral Hospital, Kenya, on treatment for abdominal tuberculosis, had laparotomy for peritonitis with bowel resection then subsequently developed intra-abdominal abscess. Re-do laparotomy showed a break-down of the anastomosis with generalized purulent contamination so Ileostomy was fashioned in the midline wound following which he developed a burst abdomen with concomitant fistula (Figure 1). After a CT scan for the abdomen ruling out further collections, the patient was treated as per sepsis protocol, commenced total parenteral nutrition, the wound was then debrided and fitted with appropriately fitting wound pouch bag (Eakin Wound Pouch) with an opening at the centre for the fistulae and stoma to drain.

Figure 1: The completely open abdomen with fistulas and ileostomy, extensive skin excoriations.

Figure 2: Application of a large wound pouch bag with a reservoir.
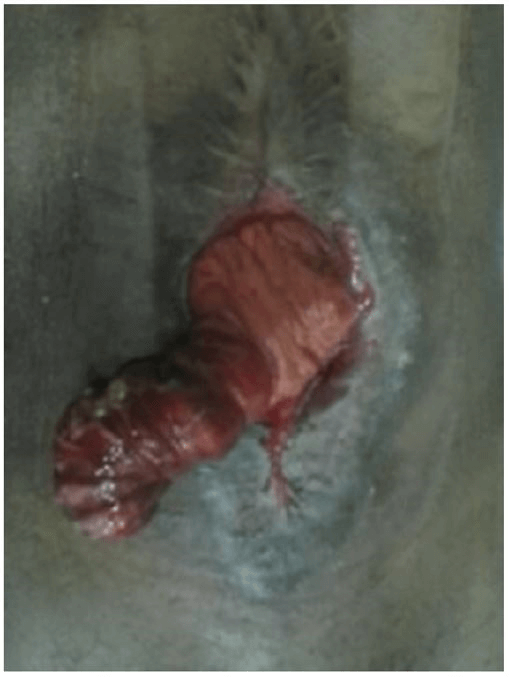
Figure 3: Wound significantly granulated and contracted at 6 weeks. Distal limb of ileostomy prolapsed through the wound.

Figure 4: Wound after ileostomy reversal, well healed with a slight dehiscence of the skin.
The pouch also had a bag to collect enteric fluid and determine their accurate output and guide in the replacement of losses (Figure 2). This pouch was changed once weekly, as the wound granulated well and contracted to near healing by 6 weeks (Figure 3). After 4 months, when the patient’s nutrition improved, Ileostomy was reversed and this left the patient only with a superficially dehisced skin which fully healed after being dressed with saline gauze (Figure 4). The patient completed his anti-TB chemotherapy at 9 months and was discharged from follow-up.
Conclusion
The wound pouch might be a simple and effective way in controlling fistula and ileostomy drainage which could be used for complex fistulas. It limits skin corrosion and stimulates wound granulation and contraction. It also enhances patient comfort, enable patient mobility and contain the cost of care as it has reduced hospital stay significantly and reduced overall time to healing.
Article Info
Article Type
Case ReportPublication history
Received: Fri 05, Jun 2020Accepted: Thu 02, Jul 2020
Published: Tue 07, Jul 2020
Copyright
© 2023 Abdirahaman Nuno. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.AJSCR.2020.03.05
Figures & Tables
References
- Cem Terzi, Tufan Egeli, Aras E Canda, Naciye C Arslan (2014) Management of enteroatmospheric fistulae. Int Wound J 11: 17-21. [Crossref]
- Stephen Girard, Matthew Sideman, David A Spain (2002) A novel approach to the problem of intestinal fistulization arising in patients managed with open peritoneal cavities. Am J Surg 184: 166-167. [Crossref]
- Pedro G R Teixeira, Kenji Inaba, Joseph Dubose, Ali Salim, Carlos Brown et al. (2009) Enterocutaneous fistula complicating trauma laparotomy: a major resource burden. Am Surg 75: 30-32. [Crossref]
- William P Schecter, Rao R Ivatury, Michael F Rotondo, Asher Hirshberg (2006) Open abdomen after trauma and abdominal sepsis: A strategy for management. J Am Coll Surg 203: 390-396. [Crossref]
- https://www.eakin.eu/wound-care : What are Eakin Fistula & Wound Pouches
- Brian Layton, Joe Dubose, Shawnn Nichols, James Connaughton, Tracy Jones et al. (2010) Pacifying the open abdomen with concomitant intestinal fistula: a novel approach. Am J Surg 199: e48-e50. [Crossref]