Laparoscopic Treatment of De Garengeot´s Hernia with Appendicitis
A B S T R A C T
Introduction: The Garengeot’s hernia is a rare femoral hernia and its diagnosis should be suspected when we identified a bulging in the right iliac fossa associated with anorexia and signs of inflammation. Their treatment is still subject to divergences, and there is no common opinion about its treatment.
Presentation of Case: Female patient, LAT, 60 years old, had come to Grajau General Hospital (GGH) at the Emergency Room (ER) presenting abdominal pain localized in the right iliac fossa. Computerized tomography showed femoral hernia at right with mesenteric fat, cecal appendix and lymphonodes that suggested regional inflammatory process. The patient was submitted to a laparoscopic surgery with closure of the hernia ring without the placement of a mesh.
Conclusion: The laparoscopic approach can be used as less invasive method of treatment and it presents better results.
Keywords
Garengeot, hernia, appendicitis
Introduction
Inguino-femoral hernias have a prominence within medicine, either by its frequency or by the notorious clinical involvement, whose repercussion in some cases can be serious [1]. Among the inguino-femoral hernias, rares hernias named Amyand and Garengeot, are considered less than 1% of all hernias in the anterolateral wall [2]. Considering all rare hernias, the Garengeot’s hernia stands out, in terms of clinical importance. This type of hernia consists of the vermiform appendix contained in the femoral hernia sac, representing 0,9% of the cases, only discovered accidentally during surgery for femoral hernia treatment [2, 3].
As part of the hernia, the appendix might suffer all type of inflammation process, which can lead to acute appendicitis, however it’s not usual, representing only 0,08-0,13%, as seem in the literacture, hindering it diagnosis [2]. The acute appendicitis in Garengeot’s hernia prevails in women (13:1, 93% of women), as well as had been increasing the number of femoral hernias in those population, and the frequency increases after menopause, occurring in elderly patients of 70 years in average [4-7]. Studies suggest that the rare occurrence of this kind of hernia can be caused by abnormal anatomic position of the appendix, due to an intestinal rotation in different degrees during embryonic development or sorted cecum fixation. A cecum with bigger anatomy than normal, which extends itself until the pelvis, might allow the entrance of the appendix in the hernia bag. If there´s a compression of the femoral hernia neck, choking it, then it has an evidence of acute appendicitis, and perforation might be seen [5].
The diagnosis for Garengeot’s hernia can be explained for, firstly, the clinical condition of the patient itself, represented by signs and symptoms closer to an incarcerated inguinal or femoral hernia, such as pain and erythematous mass in crotch area. The peritonitis is not usual for this condition due to isolation of the appendix in hernia sac which this way it doesn’t touch the peritoneal cavity [3, 8]. The methods for image investigation of the Garengeot’s hernia are inefficient. The radiography of abdomen might show obstruction of the small bowel, meanwhile the tomography might not present the appendix in the hernia bag. The ultrasonography can also be an option once it shows the presence of herniation of the appendix through the femoral canal and inflammatory signs of acute appendicitis too, however, only through surgery this type of hernia might be confirmed [9, 10].
The treatment for Garengeot’s hernia depends of the situation of the appendix. If it’s not inflamed, the surgery consists in reduce it to the peritoneal cavity, followed by correction of the femoral ring fail. However, in the presence of any stage of acute appendicitis it’s necessary to remove the appendix followed by correction of the femoral ring. The surgical approach using a mesh is controversial, not being fully indicated due to relative risk of infection in the surgical site. Still, some studies show absolute contraindication only in cases of local abscess or organ drilling [3, 11]. Argudo et al. consider the correction of the abdominal wall using mesh in case of infection is safe and other studies show that it’s not the use of this material into the cavity that would cause damage, but the time for surgical intervention. But literature itself still shows that, due to only few evidences, the safest method is not using the mesh for cases of acute appendicitis in Garengeot’s hernia [12-14].
Case Description
Female patient, LAT, 60 years old, had come to Grajau General Hospital (GGH) at the Emergency Room (ER) on February 10th, 2018 complaining about pain in right inguinal area for 4 days, with no irradiation, in compression, and no side factors. She had already looked for previous medical assistance, in which she was medicated and dismissed due to improvement in her clinical condition. Appeared in the service in worst condition, presenting bulging in right inguinal area, followed by pain, fever for the last day, anorexia, loss of appetite and nauseas.
As personal background, the patient denied comorbidities but confirmed smoking of 40 packs/year. Laboratory and image exams were held and for laboratory no left deviation or leukocytosis were shown. In the tomography there was evidence of right femoral hernia with mesenteric fat and cecal, and association of densification of adjacent fat planes with the increase of the number of inguinal lymph nodes in this side, suggesting regional inflammatory process. As conduct, it was applied surgical treatment by laparoscopy to correct the right femoral hernia. During surgery, it was possible to see the presence of femoral hernia with a strangulated hernia bag having a cecal appendix with mesenteric fat at in its content (Figure 1).
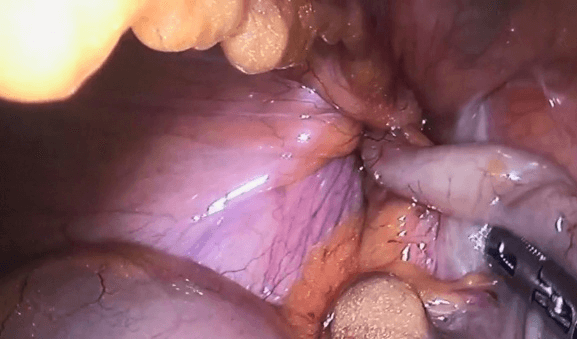
Figure 1: Laparoscopic view of femoral hernia with a strangulated appendix.
At first, an attempt of undo the strangled was applied, but it has no success. It was chosen, in the following, to make a flap dissection of the peritoneum in lateral direction with straight isolation of the hernia bag, it was identified the cecal appendix basis and accomplished double ligature with cotton 2-0, with cauterization and dissection of the mesoappendix. After the recognition steps, the hernial ring was enlarged and posteriorly removed from the cecal appendix. The appendix was classified with perforation in its structure, without presence of local pus and adjacent fat (Figure 2).
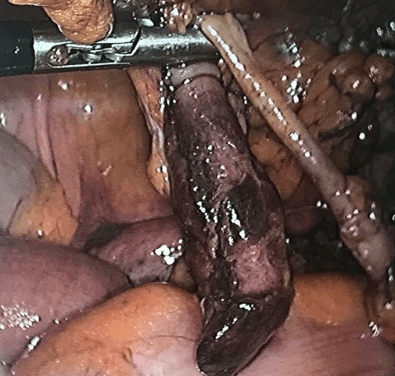
Figure 2: Appendix was classified with perforation in its structure, without presence of local pus.
Finally, the hernia ring was closed, with the iliopubic tract approaching and Cooper's ligament with Dexon 2-0 thread, with two U-points, opting not to place the mesh due to local inflammatory activity. Peritoneal flap raffia was performed with Dexon 2-0, with continuous stitches, removing the sectioned cecal appendix between ligatures, with exteriorization by the portal of 10 mm. The procedure was performed without intercurrences (Figure 3). Patient is in clinical follow-up for 12 months without evidence of hernia recurrence or any other complication.
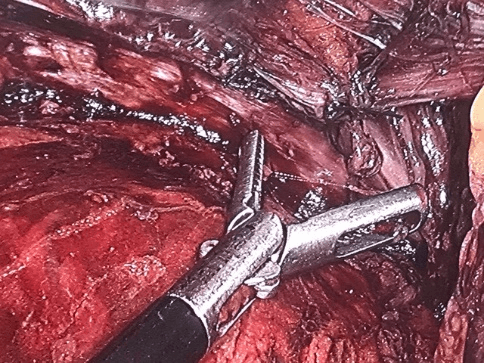
Figure 3: The hernia ring was closed, with the iliopubic tract approaching and Cooper's ligament with Dexon 2-0, with two U-points.
Discussion
The Inguino-femoral hernias stand out because they are conditions that, if not treated in their acute stage, might cause severe consequences [1]. Among the inguino-femoral hernias, the Garengeot’s hernia is considered a rare form of femoral hernia [2]. This kind of hernia was described for the first time by French surgeon René Jacques Croissant de Garengeot (1688-1759) and since then its diagnosis is challenging, even with patient’s clinical and complementary exams, such as image methods of diagnosis. Besides that, the treatment applied to this condition is still divergent, without consensus [15].
In Literature there are no consensus between incisional and laparoscopic ways of treatments [15, 16]. The inguinal incision is used in 48% of the cases, the low median laparotomy is used in 10% of the cases, the laparoscopic turned into inguinotomy in 5% of cases and vertical over the femoral incision in only 3% of the cases. The major challenge is the approach of the appendix depending on the anatomy and position of the cecum [17]. The laparoscopic approach is an option of technic, in which the surgeon is sure about the diagnosis and might explore the abdominal cavity better and in first place [8].
Conclusion
The Garengeot’s hernia is a differential, unusual, diagnosis in patients that present suggestive clinical signs of strangled femoral hernia. The laparoscopic surgery might be applied as a less invasive method and with better resolution.
Article Info
Article Type
Case ReportPublication history
Received: Fri 08, May 2020Accepted: Tue 19, May 2020
Published: Mon 25, May 2020
Copyright
© 2023 Murillo De Lima Favaro. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.AJSCR.2020.02.08
Figures & Tables
References
- Goulart A, Martins S (2015) Hérnia Inguinal: Anatomia, Patofisiologia, Diagnóstico e Tratamento. Rev Port Cir 33: 25-42.
- Simons MP, Smietanski M, Bonjer HJ, Bittner R, Miserez M et al. (2018) International guidelines for groin hernia management. Hernia 22: 1-165. [Crossref]
- Sharma H, Jha PK, Shekhawat NS, Memon B, Memon MA (2007) De Garengeot hernia: an analysis of our experience. Hernia 11: 235-238. [Crossref]
- Rajan SS, Girn HR, Ainslie WG (2009) Inflamed appendix in a femoral hernial sac: de Garengeot's hernia. Hernia 13: 551-553. [Crossref]
- Nguyen ET, Komenaka IK (2004) Strangulated femoral hernia containing a perforated appendix. Can J Surg 47: 68-69. [Crossref]
- Corder AP (1992) The diagnosis of femoral hernia. Postgrad Med J 68: 26-28. [Crossref]
- Ebisawa K, Yamazaki S, Kimura Y, Kashio M, Kurito K et al. (2009) Acute Appendicitis in an Incarcerated Femoral Hernia: A Case of De Garengeot Hernia. Case Rep Gastroenterol 3: 313-317. [Crossref]
- Thomas B, Thomas M, McVay B, Chivate J (2009) De Garengeot hernia. JSLS 13: 455-457. [Crossref]
- Gurer A, Ozdogan M, Ozlem N, Yildirim A, Kulacoglu H et al. (2006) Uncommon content in groin hernia sac. Hernia 10: 152-155. [Crossref]
- Ramos KVF, Cruz FCS, Souza Filho JC, Fukushima M, Monteiro MB (2016) Apendicite aguda em hérnia de garengeot. Rev Col Bras Cir 2: 1-2.
- Zissin R, Brautbar O, Shapiro Feinberg M (2000) CT diagnosis of acute appendicitis in a femoral hernia. Br J Radiol 73: 1013-1014. [Crossref]
- Argudo N, Pereira JÁ, Sancho JJ, Membrilla E, Pons MJ et al. (2014) Prophylactic synthetic mesh can be safely used to close emergency laparotomies, even in peritonitis. Surgery 156: 1238-1244. [Crossref]
- Jim Z, Imtiaz MR, Nnajiuba H, Samlalsingh S, Ojo A (2016) De Garengeot’s Hernia: Two Case Reports with Correct Preoperative Identification of the Vermiform Appendix in the Hernia. Case Rep Surg 2016: 2424657. [Crossref]
- Anca AV, Álvarez JLM, Campos CM, Sanz IG, Valdueza JD (2016) Apendicitis aguda perforada en una hernia femoralincarcerada: una rara forma de presentaciónde una hernia de De Garengeot. Rev Hipanoam Hernia 4: 123-126.
- Klipfel A, Venkatasamy A, Nicolai C, Roedlich MN, Veillon F et al. (2017) Surgical management of a De Garengeot’s hernia using a biologic mesh: A case report and review of literature. Int J Surg Case Rep 39: 273-275. [Crossref]
- Ikran S, Kaleem A, Satyapal D, Ahmad SM (2018) De Garengeot's hernia: a rare presentation of the wandering apendix. BMJ Case Rep 2017-223605. [Crossref]
- Kalles V, Mekras A, Mekras D, Papapanagiotou I, Al Harethee W et al. (2013) De Garengeot’s hernia: a comprehensive review. Hernia 17: 177-182. [Crossref]