Intestinal Perforation by an Ingested Bone Fragment: A Case Report
A B S T R A C T
Introduction: The ingestion of a foreign body is most often accidental. The main complication is intestinal perforation. We report a case of intestinal perforation by ingestion of a bone fragment.
Case Report: It was a 45-year-old man, who was received for abdominal pain of second right flank and vomiting. Physical examination found abdominal tenderness predominant in the right lower quadrant. The CT scan showed fluid peritoneal effusion with pneumoperitoneum with a bone fragment in the lumen of the distal ileum. An intestinal resection removing the perforation followed by an end to end anastomosis was performed favorably.
Conclusion: Intestinal perforation is a serious complication of ingested foreign bodies. The diagnosis is improved by CT scan. The treatment is surgical.
Keywords
Foreign body, peritonitis, emergency, surgery, computed tomography
Introduction
Intestinal perforation by ingested foreign bodies is rare (1%) [1]. It is oftenly due to sharp food fragments such as fish bones [2, 3]. Bone fragments are rarely involved. We report a case of intestinal perforation by ingestion of a bone fragment.
Case Report
It was a 45-year-old man, who was received for abdominal pain of second right flank and vomiting. These symptoms were evolving for 2 weeks. He had fever at 37.8 °C. Physical examination found abdominal tenderness predominant in the right lower quandrant. Biology showed leukocytosis at 10400/mm3. The CT scan showed fluid peritoneal effusion with pneumoperitoneum. In addition, there was a hyperdense foreign body in the lumen of the distal ileum (Figure 1). The exploration by a median laparotomy found digestive fluid estimated at 700 cc due to a perforation of distal ileum (Figure 2). We also noticed by palpation a foreign body in the intestinal lumen. An intestinal resection removing the perforation followed by an end to end anastomosis was performed. An abdominal drainage was associated. The opening of the resection specimen showed a sharp bone fragment (Figure 3). The postoperative course was marked by a surgical site infection that has well evolved after medical treatment. The patient was discharged at the 7th day.
Discussion
The foreign bodies most involved in intestinal perforations are fish bones in 63% followed by bone fragments in 17% [1]. This is explained by the sharpness of these types of foreign bodies as in our case report [4]. Some risk factors are oftenly found, such as psychiatric disorders, alcoholism, extreme ages or use of dental prosthesis [5]. No particular factor was found in our patient. Perforation can sit on the entire digestive tract. However, the preferential localization is angulation areas zones with smaller diameter such as the ileocecal valve, the recto-sigmoid junction or the terminal intestine as in our observation [6]. The existence of surgical history on the digestive tract or preexisting pathologies like diverticula or intestinal malformations can also promote the occurrence of complications [5]. In our patient, these contributing factors were not found.

Figure 1: CT scan with intra digestive hyperdense foreign body (arrow) with pneumoperitoneum (star).
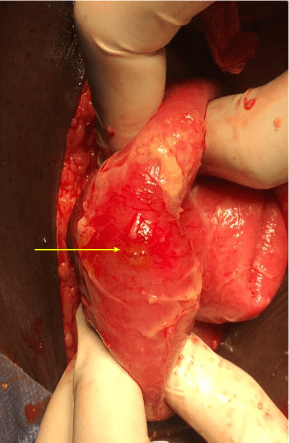
Figure 2: Per operative image showing the intestinal perforation.

Figure 3: Image showing the foreign body (sharp bone fragment).
Bowel perforation can have multiple clinical presentations. Localized or generalized peritonitis is the most frequent presentation. However, the constitution of a local intra-abdominal or parietal abscess is possible [7]. The diagnosis is based essentially on the CT scan which has a sensitivity of 100% [8]. It gives the localization and look for signs of intestinal perforation as in our case [9]. The treatment of intestinal perforation by a foreign body is surgical. The principle of the treatment is based on the extraction of the foreign body and restoring digestive continuity. The classic approach is laparotomy, but laparoscopy is possible when patients are seen early [10]. For the perforation, performing a simple suture, a resection with end to end anastomosis or stoma depends on the localization and the clinical presentation [2]. In our case, we opted for resection followed by anastomosis because of localization at the distal ileum and the localized peritonitis.
Conclusion
Intestinal perforation is a serious complication of ingested foreign bodies. Preoperative diagnosis, although difficult, is improved by CT scan. The surgical technique depends on the type of foreign body, the localization, and the diagnostic delay.
Article Info
Article Type
Case ReportPublication history
Received: Mon 09, Sep 2019Accepted: Mon 14, Oct 2019
Published: Wed 20, Nov 2019
Copyright
© 2023 Tendeng JN . This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.IJSCR.2019.02.04
Figures & Tables
References
- Emir S, Ozkan Z, Altınsoy HB, Yazar FM, Sözen S et al. (2013) Ingested bone fragment in the bowel: Two cases and a review of the literature. World J Clin Cases 1: 212‑216. [Crossref]
- Goh BK, Chow PK, Quah HM, Ong HS, Eu KW et al. (2006) Perforation of the gastrointestinal tract secondary to ingestion of foreign bodies. World J Surg 30: 372-377. [Crossref]
- Rodríguez-Hermosa JI, Codina-Cazador A, Sirvent JM, Martín A, Gironès J et al. (2008) Surgically treated perforations of the gastrointestinal tract caused by ingested foreign bodies. Colorectal Dis 10: 701-707. [Crossref]
- Eisen GM, Baron TH, Dominitz JA, Faigel DO, Goldstein JL et al. (2002) Guideline for the management of ingested foreign bodies. Gastrointest Endosc 55: 802‑806. [Crossref]
- Dai J, Kapadia CR (2019) Transverse colon perforation secondary to fish bone ingestion. J Surg Case Rep 2019: rjy368 . [Crossref]
- Ho JPK, Jameson C (2018) Small bowel perforation from foreign body ingestion: Images for Surgeons. ANZ J Surg 5. [Crossref]
- Cisse M, Kaptue EC, Seck M, Toure AO, Gueye ML et al. (2015) Colon perforation by fish bone revealed by an abscess of the left flank: A case report. Surgical Chronicles 20: 278-279.
- Akazawa Y, Watanabe S, Nobukiyo S, Iwatake H, Seki Y et al. (2004) The management of possible fishbone ingestion. Auris Nasus Larynx 31: 413-416. [Crossref]
- Drakonaki E, Chatzioannou M, Spiridakis K, Panagiotakis G (2011) Acute abdomen caused by a small bowel perforation due to a clinically unsuspected fish bone. Diagn Interv Radiol 17: 160-162. [Crossref]
- Chin EH, Hazzan D, Herron DM, Salky B (2007) Laparoscopic retrieval of intraabdominal foreign bodies. Surg Endosc 21: 1457-1457. [Crossref]