Insulinoma of Pancreas, Brief Experience at a Dedicated Surgical Oncology Department
A B S T R A C T
Introduction: Insulinoma of pancreas is a rare neuroendocrine tumor (NET). Mostly insulinomas are benign and solitary. They can have association with multiple endocrine neoplasia 1 (MEN -1). Insulinomas presents with symptoms of hypoglycemia. Most of the times the symptoms are vague and result in delay in the diagnosis and hence management. After appropriate diagnostic and localization investigations along with metastatic workup, surgery is the treatment of choice. Surgery can offer cure. Minimally invasive surgery can offer potential benefits of minimal morbidity and at least equal oncological outcomes.
Study Design: Case series.
Place and Duration of Study: Department of Surgical Oncology, Shaukat Khanam Memorial Cancer Hospital & Research Center (SKMCH&RC), from January 2011 to March 2020.
Methodology: We studied a total of five patients that presented to SKMCH&RC in the above-mentioned period. Detailed clinical information of these five patients, including sociodemographic variables, symptomatology, diagnostic and localization investigations, clinical and pathological staging, comprehensive details of surgery, postoperative course, oncological outcomes, postoperative resolution of symptoms, postoperative diabetes, prognosis and follow up duration were analysed. The record was being retrospectively retrieved from Hospital Information System (HIS) that is prospectively maintained. We are a paperless hospital and all data and record of the patient is maintained through HIS.
Results: A total of five patients presented to SKMCH&RC with a mean age of 41 (18 -80) years. The median duration of symptoms was 24 (6-60) months. Symptomatic hypoglycemia was present in all 5 (100%) of the patients. Tumor distribution in the pancreas was as follows; uncinate 1 (20%), body 1 (20%) and tail 3 (60%). All five patients (100%) were treated by surgery. Resolution of symptoms occurred in all five (100%) of the patients.
Conclusion: Insulinoma of pancreas is a rare disease with varied symptomatology, physicians shall have an index of suspicion for this disorder to aid early diagnosis that is pivotal for the management and prevention of possible fatal complications of hypoglycemia. Appropriate diagnostic and localizing investigations are required. Adequate surgery can offer cure. Minimally invasive surgery can be safely offered with equal oncological outcomes.
Keywords
Hypoglycemia, insulinoma, C-Peptide, 72-hour fasting test, minimally invasive surgery
Introduction
Insulinoma of the pancreas is a rare tumor derived from beta type pancreatic islet cells. These are rare variety of tumors with incidence of around one to four cases case per million individuals [1]. Among neuroendocrine tumors (NET) of pancreas, insulinomas are the most common [2]. Mostly, the affected population is in fourth to sixth decade of life [3, 4]. Most insulinomas are benign and solitary [5]. Around 10% of the insulinomas can be malignant [6]. Malignant insulinomas are only differentiated from their benign counterparts on the basis of metastasis and local invasion. Histopathological differentiation on the basis of imaging and staining is very difficult and not possible in most of the cases. There can be an association with multiple endocrine neoplasia (MEN) type 1, in which the insulinomas are accompanied with anterior pituitary gland tumors and parathyroid hyperplasia. Around 6-10% of cases can have this genetic association [7, 8].
Most of the symptoms of the disease are due to hypoglycemia that includes confusion, irritability, dizziness, tachycardia and sometimes seizures. Neuroglycopenic symptoms are also commonly seen in this tumor. Whipple’s triad refers to 1) Symptoms of hypoglycemia 2) Blood glucose levels less than 50mg/dl and 3) relief of symptoms after ingestion of glucose [9-11]. Due to the diverse nature of the symptoms and the rarity of the disease, often the symptoms are either ignored by the patient or misinterpreted by physicians and it is not strange that the patient moves to different specialties for many months, before being properly diagnosed and managed.
Biochemical workup is done for the diagnosis of the disease that includes blood sugar levels, serum insulin levels and C-peptide levels. 72-hour fasting test is the investigation of choice for the diagnosis of insulinoma [12]. After diagnostic workup the next challenge that is being faced is localization of the tumor. Contrast enhanced Computerized Tomography (CT) scan is usually the first investigation of choice and has sensitivity of 56-70%. Magnetic Resonance (MR) scan can also be used with varied success rates. Endoscopic Ultrasound (EUS) is a very useful modality for the localization of the tumor as well as its ability to combine fine needle aspiration (FNA) to obtain cytology specimens. EUS has detection rates of 86.6-92.3% [13, 14]. Other invasive procedures such as angiography and arterial stimulation venous sampling (ASVS) can be used further for the localization in difficult cases [15].
Surgical excision is the treatment of choice. However, the management depends on multiple factors such as the location of the tumor in the gland, proximity to the ductal system and whether its single or multiple. For lesions that are either malignant, relatively large sized, in close proximity to ductal system or located in head of pancreas, pancreaticoduodenectomy is needed. Smaller lesions in this region and away from ductal system can be treated with enucleation. For lesions of body and tail similarly either distal pancreatectomy or enucleation depending on similar factors can be warranted [16]. Minimally invasive surgery has revolutionized the management of hepatobiliary surgery in high volume centers. Laparoscopic and robotic surgery can safely be used for the management of insulinomas with benefits of minimal invasive surgery and at least equal oncological outcomes. Minimally invasive surgery incurs less surgical trauma and inflammation and thus results in better recovery.
Methodology
I Study Subjects
All patients with diagnosis of insulinoma that were treated at Department of Surgical Oncology were included from January, 2011 to March, 2020. A total of five patients presented with diagnosis of insulinoma of pancreas to our department. We are a paperless hospital and all record of the patients is maintained in HIS and it is prospectively maintained. The diagnostic criteria of insulinoma included the following: Clinical features, blood sugar levels < 40 mg/dl, Insulin levels > 3μmol/l and C-Peptide levels > 0.6ng/ml. Seventy-two hours fasting test was further performed for the conformation of the diagnosis. However, this test could not be completed in all patients. After diagnosis, further investigations such as contrast enhanced CT scan, MR scan and EUS were further used to localize the lesion.
II Study Methods
It was a retrospective case series with convenient sampling. We retrospectively analysed the detailed clinical information of these five patients, including socio-demographic variables, symptomatology, diagnostic and localization investigations, clinical and pathological staging, comprehensive details of surgery, postoperative course, oncological outcomes, postoperative resolution of symptoms, postoperative diabetes, prognosis and follow up duration.
III Biochemical Analysis
Serum glucose levels, Insulin levels and C-Peptide were conducted at the biochemical laboratory of Shaukat Khanam Memorial Cancer Hospital and Research Centre. 72 hour fasting test was conducted while patients were being admitted in the hospital. After conformation of the clinical symptoms and biochemical criteria, the diagnosis of insulinoma was made.
IV Data Analysis
Continuous data were expressed as median and interquartile range (IQR). Categorical variables were expressed as frequencies and percentages. Data analysis was performed by SPSS version 26 for MAC.
V Institutional Review Board
Study was approved by institutional review board of SKMH&RC.
Results
A total of five patients were retrieved from HIS of SKMH&RC for inclusion in the study. In (Table 1) the demographic, clinical and diagnostic variables are described statistically. The patients included two males (40%) and three females (60%). The median age at the diagnosis was 41 (18-80) years. The median duration of symptoms before diagnosis was 24 (6-60) months. Symptomatic hypoglycemia was present in all patients.
Table 1: Demographic, clinical & diagnostic variables.
|
Age, Median (IQR) |
41 (18 -80) |
|
Gender, n (%) Male Female |
2 (40) 3 (60) |
|
Duration of symptoms before resection (months) (IQR) |
24 (6 – 60) |
|
Symptomatic hypoglycemia Neurological symptoms |
5 (100) 3 (60) |
|
Blood Glucose levels fasting (mg/dl) IQR |
27 (24-40) |
|
Insulin levels μU/mL (IQR) |
29 (25-38) |
|
72- hour fasting test n (%) (performed in Four patients only) |
4 (100) |
|
C-Peptide levels ng/ml (IQR) |
8.43 (1.74 -9.65) |
|
Localization of lesion in pancreas, n (%) Uncinate Body Tail |
1(20) 1 (20) 3 (60) |
|
Maximum dimension of tumor cm <2cm >2cm |
4 (80) 1 (20) |
|
Focality Unifocal Multifocal |
5(100) 0 (0%) |
|
Metastasis at presentation, n (%) |
0 (0) |
|
|
|
|
Ki – 67 index <2% 2-20% >20% |
4 (80) 1 (20) 0 (0) |
|
Synaptophysin n (%) Chromogranin n (%) |
5 (100) 4 (80) |
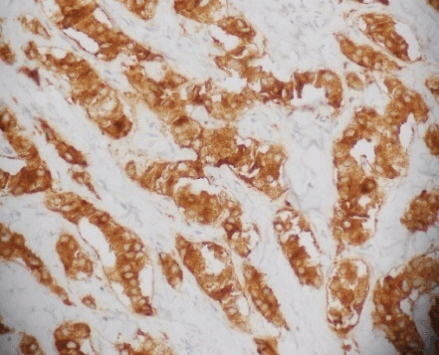
Figure 1: Synaptophysin stain showing tumor cells staining positive for synaptophysin.
As regards to the tumor distribution in the pancreas, the following distribution was observed; uncinate 1 (20%), body 1 (20%) and tail 3 (60%). No patient had metastasis at presentation. Figure 1 shows synaptophysin positivity that was taken from the record of one of the patients. Similarly, Figure 2 shows K-67 index that was retrieved from the record of one of our patients.
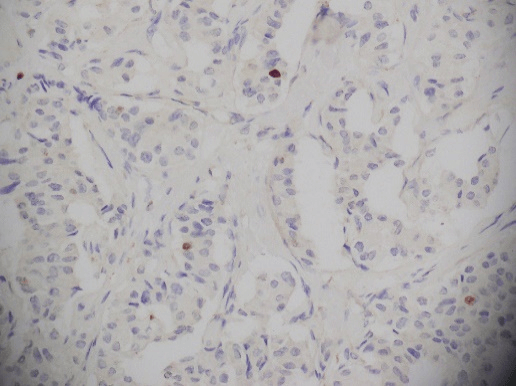
Figure 2: Ki-67 index.
Table 2: Intraoperative and post-operative outcomes.
|
Approach n (%) Open Lap converted to open 3-D laparoscopic |
2 (40) 1 (20) 2 (40) |
|
Procedure n (%) Whipple’s procedure Distal Pancreatectomy and splenectomy Enucleation |
1 (20) 3 (60) 1 (20) |
|
Blood loss (ml) Median (IQR) |
50 (25 – 150) |
|
Duration of surgery (minutes) Median (IQR) |
230 (150 – 360) |
|
ICU stay (days) Median (IQR) |
0 (0 –2) |
|
Stay in hospital (days) Median (IQR) |
5 (4 - 8) |
|
90-day mortality |
0 (0%) |
|
Resolution of symptoms, n (%) |
5 (100) |
|
Appearance of post-operative diabetes, n (%) |
2 (40) |
In (Table 2) intra operative and post-operative outcomes are being described. Two patients (40%) underwent open surgery, 1 (20%) had laparoscopic converted to open procedure and the remaining 2 (40%) had 3-D laparoscopic resection. Whipple’s procedure was done on 1 (20%), Enucleation was done for 1 (20%) and distal pancreatectomy & splenectomy was performed for 3 (60%) patients. There was no Ninety-day mortality. In (Table 3) individual patient characteristics and details along with their overall prognosis and follow up are being described already statically. All our patients had regular follow ups as per schedule in the outpatient.
Table 3: Clinical and management variables of five patients of insulinoma.
|
Variables |
Case 1 |
Case 2 |
Case 3 |
Case 4 |
Case 5 |
|
Age |
56 |
18 |
80 |
41 |
35 |
|
Gender |
Male |
Male |
Female |
Male |
Female |
|
Duration of Symptoms (months) |
60 |
6 |
15 |
24 |
28 |
|
Neuroglycopenic Symptoms |
Yes |
Yes |
Yes |
Yes |
Yes |
|
Glucose (mg/dl) |
40 |
25 |
32 |
27 |
24 |
|
Insulin |
25 |
29 |
32 |
38 |
27 |
|
C-peptide (ng/ml) |
9.65 |
1.74 |
9.21 |
5.63 |
8.43 |
|
72-h fasting |
Not done |
Positive |
Positive |
Positive |
Positive |
|
Size (mm) |
15 x 20 |
17 x 15 |
18 x 20 |
23 x 18 |
19 x 17 |
|
Location |
Tail |
Uncinate |
Tail |
Body |
Tail |
|
Metastasis |
No |
No |
No |
No |
No |
|
Procedure |
DP + Sa |
Whipple |
DP + S |
DP + S |
Enucleation |
|
Approach |
Laparoscopic |
Open |
3-D Laparoscopic |
3-D Laparoscopic |
Open |
|
Blood loss (ml) |
30 |
150 |
25 |
100 |
50 |
|
Duration of surgery (minutes) |
230 |
300 |
180 |
360 |
150 |
|
ICU Stay (days) |
2 |
0 |
1 |
0 |
0 |
|
Duration of stay (days) |
5 |
8 |
4 |
4 |
5 |
|
Resolution of symptoms |
Yes |
Yes |
Yes |
Yes |
Yes |
|
Post-operative diabetes |
No |
No |
Yes |
Yes |
No |
|
Prognosis |
Dead |
Alive |
Alive |
Alive |
Alive |
|
Survival time (days) |
2920 |
360 |
240 |
90 |
3285 |
Discussion
Insulinoma of pancreas is a rare but most common functional pancreatic neuroendocrine tumor. We are a dedicated cancer center of Pakistan and receive referrals from all over the country. The low case volume of this tumor at our institute in the said period, is in keeping with the low incidence of the disease. Female patients accounted for 60% of the patients that is in keeping with the literature. Median age was 41 (18-80) years. The median age reported in our study is in keeping with internationally published data, that states the most frequent age group effected to be fourth decade of life [3, 4]. However, the patients at extremes of age were atypical in terms of published age distribution of the tumor. One patient presented in second decade of life and another presented in the Eighth decade of life in our studied cohort. Documentation of Whipple’s triad is of paramount importance for the diagnosis of insulinoma [17].
In our study the symptoms of Whipple’s triad were manifested in all 5 (100%) of the patients. That is more as compared to published data as in some series up to 77% of the patients have classical manifestations of Whipple’s triad. The final diagnosis at our department was made by 72hours fasting test that is sensitive and specific for the diagnosis of insulinoma. However, the test was not possible in one patient as she was 80 years old and frail and could not tolerate prolonged fasting. All patients in our study group had benign insulinomas, that is in keeping with the published data that incidence of malignant insulinomas is extremely rare. This low percentage of malignant cases in our series could also be because of very small study population. Four patients presented with small lesions < 2cm and all were unifocal. That is in keeping with the published data. In most of the patients, the lesions were located in the tail of the pancreas that is in keeping with the published data [18].
Among non-invasive localizing investigations ultrasound has a low sensitivity of 9-64% [1]. CT scan and MR scan can yield sensitivities of 56-70% and 63-86%. As regards to invasive localization techniques [1]. EUS has detection rates of 86.6-92.3 % [13, 14]. We at our institute routinely perform EUS for the diagnosis and management of these tumors. Laparoscopic ultrasound can further aid in the localization of the tumor [19]. Laparoscopic ultrasound is selectively used at our institute for the management of pancreatic lesions including insulinomas. Surgery is the management of choice and if adequately performed can lead to cure of the patient. It can lead to a resolution of symptoms in 95% of the patients, however in our series all patients (100%) had resolution of their symptoms. Surgery for pancreas has moved all the way from open surgery to minimally invasive surgery. In high volume centers, minimally invasive surgery for pancreatic lesions including insulinomas can be performed with minimal morbidity and at least equal oncological outcomes [20].
Conclusion
Insulinoma of the pancreas is a rare disease. There shall be high index of suspicion for this disorder in symptomatic individuals. Prompt diagnosis and management are pivotal in treating this disorder. Appropriate diagnostic and localizing investigations shall be performed. Surgery is the cornerstone of treatment and if adequately done can lead to cure.
Study Limitations
Our study had limitations of smaller sample size, retrospective nature and long span of the study duration; from 2011 to 2020 which can imply non-uniformity in the diagnostic and therapeutic management options.
Author Contributions
All the authors mentioned above have contributed substantially to each of the mentioned below:
• Concept and design of study or acquisition of data or analysis and interpretation of data.
• Drafting the article or revising it critically for important intellectual content.
• Final approval of the version to be published.
Funding
None.
Ethical Approval
Ethical approval was obtained from Institutional review board (IRB) of SKMH&RC.
Competing Interests
None.
Conflicts of Interest
None.
Disclosure
The author and co-authors have no disclosures.
Article Info
Article Type
Research ArticlePublication history
Received: Mon 13, Jul 2020Accepted: Fri 24, Jul 2020
Published: Mon 10, Aug 2020
Copyright
© 2023 Aun Jamal. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.COR.2020.08.10
Figures & Tables
Table 1: Demographic, clinical & diagnostic variables.
|
Age, Median (IQR) |
41 (18 -80) |
|
Gender, n (%) Male Female |
2 (40) 3 (60) |
|
Duration of symptoms before resection (months) (IQR) |
24 (6 – 60) |
|
Symptomatic hypoglycemia Neurological symptoms |
5 (100) 3 (60) |
|
Blood Glucose levels fasting (mg/dl) IQR |
27 (24-40) |
|
Insulin levels μU/mL (IQR) |
29 (25-38) |
|
72- hour fasting test n (%) (performed in Four patients only) |
4 (100) |
|
C-Peptide levels ng/ml (IQR) |
8.43 (1.74 -9.65) |
|
Localization of lesion in pancreas, n (%) Uncinate Body Tail |
1(20) 1 (20) 3 (60) |
|
Maximum dimension of tumor cm <2cm >2cm |
4 (80) 1 (20) |
|
Focality Unifocal Multifocal |
5(100) 0 (0%) |
|
Metastasis at presentation, n (%) |
0 (0) |
|
|
|
|
Ki – 67 index <2% 2-20% >20% |
4 (80) 1 (20) 0 (0) |
|
Synaptophysin n (%) Chromogranin n (%) |
5 (100) 4 (80) |
Table 2: Intraoperative and post-operative outcomes.
|
Approach n (%) Open Lap converted to open 3-D laparoscopic |
2 (40) 1 (20) 2 (40) |
|
Procedure n (%) Whipple’s procedure Distal Pancreatectomy and splenectomy Enucleation |
1 (20) 3 (60) 1 (20) |
|
Blood loss (ml) Median (IQR) |
50 (25 – 150) |
|
Duration of surgery (minutes) Median (IQR) |
230 (150 – 360) |
|
ICU stay (days) Median (IQR) |
0 (0 –2) |
|
Stay in hospital (days) Median (IQR) |
5 (4 - 8) |
|
90-day mortality |
0 (0%) |
|
Resolution of symptoms, n (%) |
5 (100) |
|
Appearance of post-operative diabetes, n (%) |
2 (40) |
Table 3: Clinical and management variables of five patients of insulinoma.
|
Variables |
Case 1 |
Case 2 |
Case 3 |
Case 4 |
Case 5 |
|
Age |
56 |
18 |
80 |
41 |
35 |
|
Gender |
Male |
Male |
Female |
Male |
Female |
|
Duration of Symptoms (months) |
60 |
6 |
15 |
24 |
28 |
|
Neuroglycopenic Symptoms |
Yes |
Yes |
Yes |
Yes |
Yes |
|
Glucose (mg/dl) |
40 |
25 |
32 |
27 |
24 |
|
Insulin |
25 |
29 |
32 |
38 |
27 |
|
C-peptide (ng/ml) |
9.65 |
1.74 |
9.21 |
5.63 |
8.43 |
|
72-h fasting |
Not done |
Positive |
Positive |
Positive |
Positive |
|
Size (mm) |
15 x 20 |
17 x 15 |
18 x 20 |
23 x 18 |
19 x 17 |
|
Location |
Tail |
Uncinate |
Tail |
Body |
Tail |
|
Metastasis |
No |
No |
No |
No |
No |
|
Procedure |
DP + Sa |
Whipple |
DP + S |
DP + S |
Enucleation |
|
Approach |
Laparoscopic |
Open |
3-D Laparoscopic |
3-D Laparoscopic |
Open |
|
Blood loss (ml) |
30 |
150 |
25 |
100 |
50 |
|
Duration of surgery (minutes) |
230 |
300 |
180 |
360 |
150 |
|
ICU Stay (days) |
2 |
0 |
1 |
0 |
0 |
|
Duration of stay (days) |
5 |
8 |
4 |
4 |
5 |
|
Resolution of symptoms |
Yes |
Yes |
Yes |
Yes |
Yes |
|
Post-operative diabetes |
No |
No |
Yes |
Yes |
No |
|
Prognosis |
Dead |
Alive |
Alive |
Alive |
Alive |
|
Survival time (days) |
2920 |
360 |
240 |
90 |
3285 |
References
- Okabayashi T, Shima Y, Sumiyoshi T, Kozuki A, Ito S et al. (2013) Diagnosis and management of insulinoma. World J Gastroenterol 19: 829-837. [Crossref]
- Pasieka JL, McLeod MK, Thompson NW, Burney RE et al. (1992) Surgical approach to insulinomas. Assessing the need for preoperative localization. Arch Surg 127: 442-447. [Crossref]
- Service FJ, McMahon MM, O’Brien PC, Ballard DJ (1991) Functioning insuli- noma--incidence, recurrence, and long-survival of patients: a 60-year study. Mayo Clin Proc 66: 711-719. [Crossref]
- Cryer PE, Axelrod L, Grossman AB, Heller SR, Montori VM et al. (2009) Endocrine Society. Evaluation and man- agement of adult hypoglycemic disorders: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 94: 709-728. [Crossref]
- Service FJ, McMahon MM, O’Brien PC, Ballard DJ (1991) Functioning insulinoma incidence, recurrence, and longterm survival of patients: a 60 year study. Mayo Clin Proc 66: 711-719. [Crossref]
- Baudin E, Caron P, Lombard Bohas C, Tabarin A, Mitry E et al. (2013) Malignant insulinoma: recommendations for characterisation and treatment. Ann Endocrinol (Paris) 74: 523-533. [Crossref]
- Kulke MH, Bergsland EK, Yao JC (2009) Glycemic Control in Patients with Insulinoma Treated with Everolimus. N Engl J Med 360: 195-197. [Crossref]
- Edge SB, Byrd DR, Compton CC (2010) AJCC (American Joint Committee on Cancer) Cancer Staging Manual, 7th ed, Springer, New York Vol 2010: 241.
- Placzkowski KA, Vella A, Thompson GB, Grant CS, Reading CC et al. (2009) Secular trends in the presentation and management of functioning insulinoma at the Mayo Clinic, 1987-2007. J Clin Endocrinol Metab 94: 1069-1073. [Crossref]
- Service FJ, Dale AJ, Elveback LR, Jiang NS (1976) Insulinoma: clinical and diagnostic features of 60 consecutive cases. Mayo Clin Proc 51: 417-429. [Crossref]
- Dizon AM, Kowalyk S, Hoogwerf BJ (1999) Neuroglycopenic and other symptoms in patients with insulinomas. Am J Med 106: 307-310. [Crossref]
- Rostambeigi N, Thompson GB (2009) What should be done in an operating room when an insulinoma cannot be found? Clin Endocrinol (Oxf) 70: 512-515. [Crossref]
- Sotoudehmanesh R, Hedayat A, Shirazian N, Shahraeeni S, Ainechi S et al. (2007) Endoscopic ultrasonography (EUS) in the localization of insulinoma. Endocrine 31: 238-241. [Crossref]
- Goh BK, Ooi LL, Cheow P, Tan Y, Ong H et al. (2009) Accurate preoperative localization of insulinomas avoids the need for blind resection and reoperation: analysis of a single institution experience with 17 surgically treated tumors over 19 years. J Gastrointest Surg 13: 1071-1077. [Crossref]
- Morita S, Machida H, Kuwatsuru R, Saito N, Suzuki K et al. (2007) Preoperative localization of pancreatic insulinoma by super selective arterial stimulation with venous sampling. Abdom Imaging 32: 126-128. [Crossref]
- Finlayson E, Clark OH (2004) Surgical treatment of insulinomas. Surg Clin North Am 84: 775-785. [Crossref]
- Shin JJ, Gorden P, Libutti SK (2010) Insulinoma: pathophysiology, localization and management. Future Oncol 6: 229-237. [Crossref]
- Kuzin NM, Egorov AV, Kondrashin SA, Lotov AN, Kuznetzov NS et al. (1998) Preoperative and intraoperative topographic diagnosis of insulinomas. World J Surg 22: 593-597. [Crossref]
- Li W, An L, Liu R, Yao K, Hu M et al. (2011) Laparoscopic ultrasound enhances diagnosis and localization of insulinoma in pancreatic head and neck for laparoscopic surgery with satisfactory postsurgical outcomes. Ultrasound Med Biol 37: 1017-1023. [Crossref]
- Antonakis PT, Ashrafian H, Martinez Isla A (2015) Pancreatic insulinomas: Laparoscopic management. World J Gastrointest Endosc 7: 1197-1207. [Crossref]