Idiopathic Ovarian Vein Thrombosis: A Rare Case in Nonpregnant Woman
A B S T R A C T
Ovarian vein thrombosis (OVT) is a rare cause of abdominal pain, is an entity most commonly diagnosed after pregnancy. It is also associated with gynecological malignancies, caesarean deliveries, abortions, hypercoagulability and pelvic inflammatory disease. Prompt diagnosis and treatment is warranted to avoid serious complications [1]. We report the rare case of idiopathic ovarian right vein thrombosis.
Keywords
Ovary, ovarian, venous, thrombosis, thrombus
Introduction
The ovarian vein thrombosis occurs in the right side in 70-90% of cases, and bilaterally in 11-14%. Moreover, the natural history of OVT, in terms of recurrence and expected survival, has not been well-described. The differential diagnosis of OVT includes acute appendicitis, endometritis, pelvic inflammatory disease, pyelonephritis, nephrolithiasis, tubo-ovarian abscess, and ovarian torsion CT should serve as the diagnostic modality in suspected cases [2, 3]. Thrombophilic evaluation has an important role in patients with non-pregnancy related OVT [4].
The ovarian veins originate from the venous plexus in the broad ligament and communicate with the uterine plexus. The ovarian vein on each side is in the retroperitoneum anterior to the psoas muscle. The right ovarian vein joins the inferior vena cava (IVC) below the right renal vein and the left ovarian vein drains into the left renal vein [5]. A recent study noted that the ovarian veins are best visualized at the level of the inferior mesenteric artery origin, where both veins are surrounded by retroperitoneal fat [6].
OVT may be diagnosed with ultrasonography, magnetic resonance imaging, or CT scan [1, 7]. However, high-resolution CT scan with the administration of IV contrast is currently considered the diagnostic imaging modality of choice [3, 7]. The sensitivity of CT scan is reported to be 95%, but the sensitivity of Doppler ultrasonography is only approximately 50% [3].The treatment is generally conservative – IV heparin and antibiotics – but surgery may be indicated in rare clinical pictures to treat underlying disorders [6].
Case Report
A 39-year-old woman presented to the Emergency Gynecology with six days of sharp right-sided abdominal pain, nausea and abdominal volume increase. She did not have diarrhea, dysuria, or fever. A blood count and other laboratory tests were as follows: Hb 14.1 g/dL; Ht 39.9%; leukocyte count 8950/𝜇L; MCV 85.1 fL; platelets 313000/𝜇L; serum creatinine 0.68 mg/dL. Urinary analysis was otherwise normal. Her body mass index was 30.2.
I Investigation
Laboratory investigations including protein C, protein S, antithrombin III, screening for factor Leiden V and prothrombin G20210A mutations, skin pathergy test, lupus anticoagulant, anticardiolipin antibodies, homocysteine were all tests negative (Table 1).
Table 1: Complementary laboratorial exams.
|
Exams |
Results |
|
protein S |
40% (60 to 100%) |
|
protein C |
84% (70 to 150%) |
|
homocysteine |
6 µmol/l (5 to13µmol/l) |
|
antithrombin III |
17% (75 to 120%) |
|
anticardiolipin antibody IgG |
negative |
|
anticardiolipin antibody IgM |
negative |
|
screening for prothrombin G20210A mutations (Z20210A) |
Negative to mutation |
|
screening R506Q (G1891A) for factor Leiden V |
Negative to mutation |
|
lupus anticoagulant |
Negative lupus anticoagulant |
|
skin pathergy test |
negative |
USG – Uterus in anteversion, normal limits and borders, 0.5 cm echo-endometrial, right ovary with multiple peripheral cysts (above 12 cysts) smaller than 1.0 cm, Total volume of 23.7 cc. Left ovary as multiple small cysts (above of 12 cysts) less than 1.0 cm, free sac fundus, absence of adnexal masses, appendix not characterized.
CT Scan – Right Gonadal Vein Thrombosis.
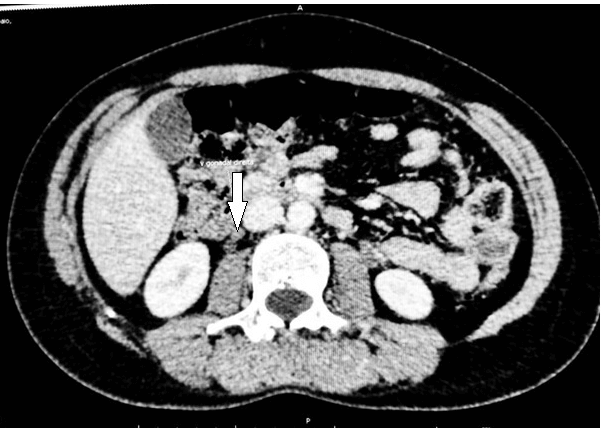
Figure 1: Complete occlusion of the right ovarian vein distal to the thrombus – CT cross section.
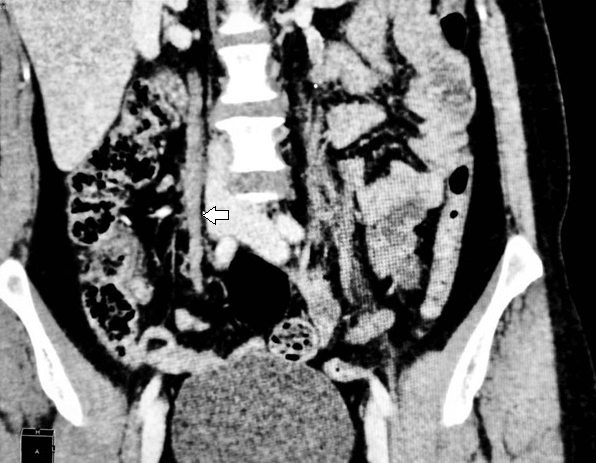
Figure 2: Complete occlusion of the right ovarian vein distal to the thrombus – CT longitudinal section.
II Diagnosis
Idiopathic ovarian vein thrombosis.
III Differential Diagnosis
Acute appendicitis and tubo-ovarian abscess were included in the differential diagnosis.
IV Treatment
Enoxaparin 6000 U, she was advised to use anticoagulant for at least 6 months.
V Outcome and Follow-Up
She was discharged with no complaints within four days. She received enoxaparin for 6 months and on follow-up free from anticoagulation with no recurrence at the 12th month of OVT but She had a thromboembolism pulmonary 24th month of OVT and now use Warfarin for anticoagulation.
Discussion
OVT is a rare cause of abdominal pain. The most frequent presentation is the triad of pelvic pain, fever and right-sided mass [8]. Often, the abdominal examination of this anatomic location closely mimics acute appendicitis [9]. Eighty percent of patients with a diagnosis of OVT present with fever. Tachycardia, nausea, and vomiting also are common [3, 9]. In this case report the patient presented with fever, nausea and the thrombus was diagnosed in the right ovarian vein.
The predisposing factors in pregnancy are thought to be venous stasis, infection and hypercoagulable state stasis [9]. Congenital pro-thrombotic conditions such as factor V Leiden, and protein S and C deficiencies may predispose an individual to OVT. Acquired prothrombotic status caused by nephrotic syndrome, antiphospholipid syndrome and chronic hematological syndrome (essential thrombocythemia) have also been reported to be associated with OVT [10]. In this rare case, we could see that the patient does not have congenital or acquired prothrombotic conditions.
Conclusion
OVT is a rare but important cause of lower quadrant abdominal pain in female patients presenting to the ED. The complications from OVT, including sepsis and pulmonary embolus, are significant. Idiopathic Ovarian Veins Thrombosis is rare, but we should always remember like a different diagnostic to abdominal pain.
Conflicts of Interest
None.
Consent
For this case report, informed consent was taken.
Funding
None.
Author Contributions
All authors contributed to the case report concept, design, review and approval of the final manuscript.
Article Info
Article Type
Case ReportPublication history
Received: Mon 30, Dec 2019Accepted: Wed 19, Feb 2020
Published: Thu 27, Feb 2020
Copyright
© 2023 Tamires de Menezes França. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.CEI.2020.01.08
Figures & Tables
Table 1: Complementary laboratorial exams.
|
Exams |
Results |
|
protein S |
40% (60 to 100%) |
|
protein C |
84% (70 to 150%) |
|
homocysteine |
6 µmol/l (5 to13µmol/l) |
|
antithrombin III |
17% (75 to 120%) |
|
anticardiolipin antibody IgG |
negative |
|
anticardiolipin antibody IgM |
negative |
|
screening for prothrombin G20210A mutations (Z20210A) |
Negative to mutation |
|
screening R506Q (G1891A) for factor Leiden V |
Negative to mutation |
|
lupus anticoagulant |
Negative lupus anticoagulant |
|
skin pathergy test |
negative |
References
- Findings DI (2005) On the AJR Viewbox. Chest 1363-1365.
- Hippach M, Meyberg R, Villena Heinsen C, Mink D, Ertan AK et al. (2000) Postpartum ovarian vein thrombosis. Clin Exp Obstet Gynecol 27: 24-26. [Crossref]
- Yildirim E, Kanbay M, Ozbek O, Coskun M, Boyacioglu S (2005) Isolated idiopathic ovarian vein thrombosis: A rare case. Int Urogynecol J Pelvic Floor Dysfunct 16: 308-310. [Crossref]
- Rottenstreich A, Da’as N, Kleinstern G, Spectre G, Amsalem H et al. (2016) Pregnancy and non-pregnancy related ovarian vein thrombosis: Clinical course and outcome. Thromb Res 146: 84-88. [Crossref]
- Sharma P, Abdi S (2012) Ovarian vein thrombosis. Clin Radiol 67: 893-898. [Crossref]
- Arslan H, Ada S, Çelik S, Toptaş T (2014) Postpartum ovarian vein and inferior vena cava thrombosis. Case Rep Med 2014: 609187. [Crossref]
- Quane LK, Kidney DD, Cohen AJ (1998) Unusual causes of ovarian vein thrombosis as revealed by CT and sonography. AJR Am J Roentgenol 171: 487-490. [Crossref]
- Doherty K, New M (2015) Idiopathic ovarian vein thrombosis in a nonperipartum patient. Obstet Gynecol 125: 1468-1470. [Crossref]
- Prieto Nieto MI, Perez Robledo JP, Rodriguez Montes JA, Garcia Sancho Martin L (2004) Acute appendicitis-like symptoms as initial presentation of ovarian vein thrombosis. Ann Vasc Surg 18: 481-483. [Crossref]
- Jacoby WT, Cohan RH, Baker ME, Leder RA, Nadel SN et al. (1990) Ovarian vein thrombosis in oncology patients: CT detection and clinical significance. AJR Am J Roentgenol 155: 291-294. [Crossref]