Granulocytic Sarcoma with Meningeal Leukemia. A Case Report
A B S T R A C T
The case of a 63-year-old woman is presented who developed 18 years after undergoing allogenic bone marrow transplantation for chronic myeloid leukaemia a granulocytic sarcoma localised in the presacral region. Complete radiologic remission was obtained with the administration of imatinib. She developed a metachron granulocytic sarcoma in the right frontal region associated to leptomeningeal infiltration. Complete clinical and near complete radiological remission was obtained with the administration of nilotinib. The patient was finally lost of progression of the frontal and meningeal localisations 45 months after the presentation of the first presacral lesion. Throughout the follow-up no sign of systemic leukaemia was detected.
Keywords
Granulosarcoma, chronic myeloid leukaemia, imatinib, nilotinib
Introduction
Granulocytic sarcoma is a rarely occurring extramedullar form of myelocytic malignancy called also myeloid sarcoma or chloroma. Usually it is a manifestation of acute myeloid leukaemia or chronic myeloid leukaemia in accelerated or blastic phase [1, 2]. A retrospective analysis found 8 granulocytic sarcomas in 615 chronic myeloid leukaemia patients [2]. Median overall survival was 14 months with tyrosine kinase inhibitors (high dose imatinib and nilotinib).
The localisation can be highly variable with soft tissues in predilection but also lymph nodes, bone, epidural region and viscera are possible [3, 4]. The diagnosis is challenging. The uncommon irregular mass can be mistaken for haematoma. The histologic examination needs special expertise.
Case Report
A 63-year-old woman was hospitalised for lumbar pain. Tonsillectomy, thymectomy, cholecystectomy, hysterectomy and bilateral ovariectomy can be revealed in her medical history. She underwent allogenic bone marrow transplantation for chronic myeloid leukaemia 18 years earlier and has been followed for a while for mild graft versus host disease. MRI showed a presacral mass. Whole body CT scan did not show any other tumoral lesion. The histologic examination of the presacral mass described immature round or ovoid cells with small cytoplasm. Immunohistochemistry showed CD117+, CD99+, CKAE1/AE3-, EMA-, CD56-, chromogranine-, MPO+, CD34 focal+, vimentin focal+, desmine-, CD3-, CD20-, CD138-, Ki67: 50%. The finding was compatible with the diagnosis of granulosarcoma (Figure 1). The diagnosis was confirmed by a second expert opinion and a positivity for Philadelphia chromosome detected with FISH.
The patient received major opioid analgesics and palliative irradiation to the sacral region. Imatinib 400 mg treatment was started and allowed a rapid clinical improvement with complete disappearance of the low back pain. The poor tolerance necessitated a dose reduction in the first step and sixteen months after treatment initiation the patient completely stopped to take the drug although, the efficacy was supported by PET CT showing no viable malignancy a year after the instauration of imatinib. Six months after having stopped to take imatinib she was complaining of frontal headache and blurred vision. Brain MRI showed a right frontal basicranial mass infiltrating the ethmoidal cellules associated to small meningeal lesions in several localisations. Liquor cytology showed elevated cell count, predominantly of lymphocytic and granulocytic type. Whole brain irradiation was discussed, but finally rejected. A treatment with nilotinib was started. Complete clinical and near complete radiological regression were obtained.
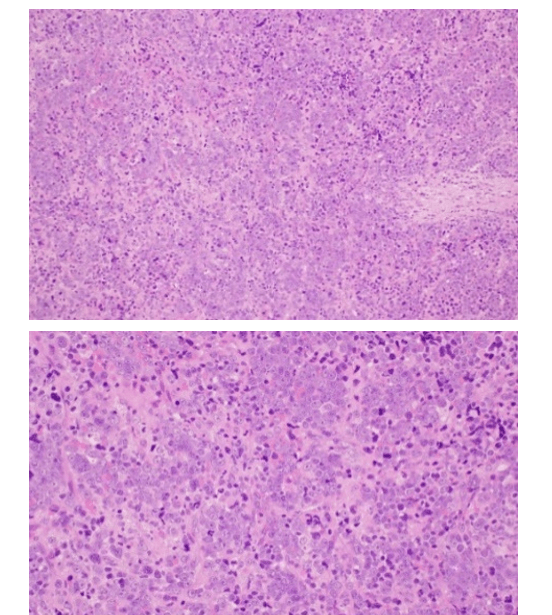
Figure 1: Histologic image of granulocytic sarcoma, a) HE stains, low and b) high magnification.
Eighteen months later, she presented with recurrent headache and vomiting. Brain MRI showed expansion of the cerebral and meningeal lesions. Liquor cytology showed again elevated cell count with 40% of blasts. Whole brain irradiation and four cycles of intrathecal cytarabine chemotherapy were given and allowed only a short clinical improvement. The patient was lost of progressing intracranial hypertension caused by uncontrolled meningeal sarcomatosis forty-five months after the diagnosis of the presacral granulosarcoma. Throughout the follow-up no sign of systemic leukaemia was detected (Figure 2).

Figure 2: Basicranial mass involving the ethmoidal cellules (a) and its near complete regression (b) after 3 months of treatment with nilotinib.
Discussion
The unique feature of this case is that granulocytic sarcoma developed independently of active leukaemia. The relatively long survival observed in this pathology of poor prognosis is probably related to the lack of systemic manifestation. The omission of cerebral irradiation upon the detection of the intracranial lesions may be discussed. We decided not to perform it because the patient’s complaints were mild and the evidences of concomitant use with tyrosine kinase inhibitors are lacking. Nilotinib allowed a significant improvement in some days. It supports the good penetration of the drug through the blood-brain barrier. At the time of progression radiotherapy was finally realised and followed by intrathecal chemotherapy without real efficacy.
Conclusion
Granulocytic sarcoma may present without associated leukaemia. The response to imatinib and nilotinib is excellent at the onset of the treatment but the long-term efficacy is shorter as compared to chronic myeloid leukaemia.
Article Info
Article Type
Case ReportPublication history
Received: Wed 11, Mar 2020Accepted: Fri 27, Mar 2020
Published: Mon 06, Apr 2020
Copyright
© 2023 Kullmann Tamás. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.RCO.2020.01.02
Figures & Tables
References
- Abir G, Ines W, Sondes M, Ramzi J, Balkis M et al. (2014) New Variant Translocation (8; 9; 21) (q22; p24; q22) in a Patient with Granulocytic Sarcoma Concurrent with Acute Myeloid Leukemia. Open J Blood Diseases 4: 43-49.
- Dasappa L, Thanky AH, Kuntegowdanahalli LC, Kanakasetty GB, Jacob LA et al. (2017) Myeloid Sarcoma as the First Sign of Progression of Chronic Myeloid Leukemia in Medullary Chronic Phase: Experience from a Tertiary Cancer Centre in Southern India. Gulf J Oncolog 1: 21-25. [Crossref]
- Zhai J, Kong X, Yang X, Gao J, Xuan L et al. (2018) An uncommon granulocytic sarcoma of the breast: a case report and literature review. Onco Targets Ther 11: 3685-3690. [Crossref]
- Ganapule AP, Viswabandya A, Jasper A, Patel P, Kokil G (2014) Granulocytic sarcoma with compressive myelopathy: a rare presentation of chronic myelogenous leukaemia. J Clin Diagn Res 8: QD03-QD04. [Crossref]