Fracture of the Femoral Component in TKR – A Case Report
A B S T R A C T
Femoral component fracture in total knee replacement (TKR) is a rare complication. In the majority of case reports, stress fractures of the femoral component have predominantly affected the medial condyle, following uncemented implantation of fixed-bearing knees. We report the case of fracture of the lateral condyle of a cemented fixed TKR due to bad cementing technique.
Keywords
Fracture, femoral component, TKR, lateral, condyle
Introduction
The failure of total knee prosthetic components is a rare event and has been most commonly reported around the polyethylene insert of tibia or the tibial prosthesis. Issues with polyethylene fracture and subsequent base plate failure are already documented [1]. Femoral component fracture in total knee replacement (TKR) is a rare complication [2-14]. The 1990s saw an increased incidence of implant fractures with the three largest series reported with the uncemented Whiteside Ortholoc II knee replacements (Dow Corning Wright, Arlington, TN, USA) [12-14]. In the majority of case reports, stress fractures of the femoral component have predominantly affected the medial condyle, following uncemented implantation of fixed-bearing knees. In this case, failure of bone ingrowth in uncemented components, higher body mass index, and a higher athletic activity led to fatigue fracture of the femoral components [9]. We report the case of fracture of the lateral condyle of a cemented TKR.
Case Report
In 2000 TKR of the left knee was performed elsewhere in a 55-year-old male patient due to posttraumatic osteoarthritis using a PFC Sigma prosthesis (DePuy Orthopaedics, Warsaw, IN, USA). 10 years later revision arthroplasty was performed due to aseptic loosening of the tibial component (Figure 1) using a PFC Sigma tibial prosthesis with a cemented intramedullary stem (Figure 2). Postoperative follow- up was uneventful. In 2017 the obese patient (BMI: 40.3) suffered from acute knee pain again. X-ray of the left knee showed loosening of the tibial component (Figure 3). Scintigraphy revealed enhancement in the region of the tibial and lateral femoral component (Figure 4). Revision arthroplasty of the left knee was recommended. Three weeks later x-ray in respect to preoperative planning showed fracture of the femoral component (Figure 5). Intraoperatively tibial and femoral component was found to be loose and the lateral condyle of the PFC Sigma prosthesis (DePuy Orthopaedics, Warsaw, IN, USA) was fractured (Figure 6) without attached of cement or bone. Fibrous tissue was found at the prosthesis bone interface around the femoral and tibial component. The cement mantle on the femoral side was incomplete. A constrained Innex SC Knee (Zimmer, Warsaw, IN, USA) was implanted (Figure 7). Postoperative follow-up was uneventful.


Figure 1: X-ray of the left knee in 2 planes: ap view (A) and lateral (B) view shows loosening of the tibial component of the PFC Sigma knee prosthesis.


Figure 2: X-ray of the left knee in 2 planes after revision surgery: ap view (A) and lateral (B) view shows a cemented tibial component with intramedullary stem.

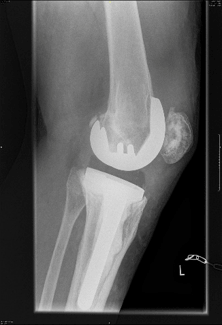
Figure 3: X-ray of the left knee in 2 planes: ap view (A) and lateral (B) view shows loosening of the tibial component but no radiolucent lines of the femoral component of the PFC Sigma knee prosthesis.

Figure 4: Scintigrapy (ap view (A) and pa view (B) reveals enhancement of the tibial and lateral femoral component of the left knee.


Figure 5: X-ray of the left knee in 2 planes: ap view (A) and lateral (B) view shows loosening of the tibial component, no radiolucent lines of the femoral component but breakage of the femoral component of the PFC Sigma knee prosthesis.
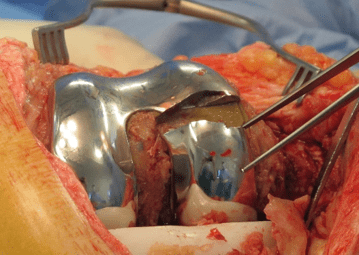
Figure 6: Intraoperative findings: Breakage of the lateral condyle of the femoral component of the PFC Knee system.
Discussion
The most common indication for revision arthroplasty of the knee is aseptic loosening (35 %) followed by infection (23 %) and pain (18 %). Component fracture represents less than 1 % of indications for revision TKR [10]. Fracture of metal implants in joint replacements is a rare but devastating complication of arthroplasty, requiring revision surgery. Fractures of the femoral component have been most widely reported in uncemented knee replacements, it’s an extremely rare condition in cemented total knee arthroplasty [2-14].


Figure 7: X-ray of the left knee in 2 planes after revision surgery: ap view (A) and lateral (B) view shows cemented constrained Innex SC Knee).
In the cases of Thompson et al., Swamy et al. and Sarraf et al., fracture of the medial condyle of a PFC SIGMA Cruciate Retaining device (DePuy Orthopaedics, Warsaw, IN, USA) occurred due to poor cementing technique [1, 10, 11]. To date, three mechanisms of femoral fatigue fracture in TKR can be postulated: Design factors, patient factors and factors exacerbating stresses. Design factors suggest inherent weaknesses in the structure of the implant, such as described with the Ortholoc II [2, 13, 14]. Patient factors include weight and varus deformity either pre- or postoperatively. Cemented devices may allow more uniform load bearing, while uncemented porous-coated prostheses often restrict bone growth to isolated areas [10]. The major patient associated risk factor for implant fatigue fracture is obesity [10].
Our patient had a normal anatomic static alignment of the total knee prosthesis but was extremely obese (BMI: 40.3) The patient suffered from acute knee pain, breakage of the femoral component was missed examining first x-rays. We follow Sarraf et al. who postulated that TKR is increasing more and more worldwide [10]. An increasing number of patients is obese at index operation. In that way component fracture is likely to become a more prevalent complication. Presently, it is a rare cause of knee pain after TKR; however, surgeons should remain vigilant and maintain a high index of suspicion with a patient who presents with acute onset pain, evidence of a varus deformity, and concomitant obesity, especially since component fractures can be easily missed on plain radiography [10]. To minimize risk of that rare complication we strongly recommend well performed modern cementing techniques and optimal leg axis in TKR [15].
Conflicts of Interest
None.
Funding
None.
Consent
The authors confirm that informed consent of the patient was taken for publication of this case report.
Article Info
Article Type
Case ReportPublication history
Received: Wed 04, Dec 2019Accepted: Sat 11, Jan 2020
Published: Sat 18, Jan 2020
Copyright
© 2023 Alexander Schuh. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.JSCR.2019.01.02
Figures & Tables
References
- Thompson SM, Railton G (2016) Catastrophic Failure of the Femoral Condylar Prosthesis in Total Knee Arthroplasty. J Orthop Trauma 6.
- Cook SD, Thomas KA (1991) Fatigue failure of noncemented porous-coated implants. A retrieval study. J Bone Joint Surg Br 73: 20-4. [Crossref]
- Duffy GP, Murray BE, Trousdale RR (2007) Hybrid total knee arthroplasty analysis of component failures at an average of 15 years. J Arthroplasty 22: 1112-1115. [Crossref]
- Han CD, Han CW, Yang IH (2009) Femoral component fracture due to osteolysis after cemented mobile-bearing total knee arthroplasty. J Arthroplasty 24: 323.e7-323.e12. [Crossref]
- Huang CH, Yang CY, Cheng CK (1999) Fracture of the femoral component associated with polyethylene wear and osteolysis after total knee arthroplasty. J Arthroplasty 14: 375-379. [Crossref]
- Lemaire R (2010) Fatigue fracture of the femoral component in a mobile bearing knee prosthesis. Acta Orthop Belg 76: 274-281. [Crossref]
- Luring C, Perlick L, Schubert T, Tingart M (2007) A rare cause for knee pain: fracture of the femoral component after TKR. A case report. Knee Surg Sports Traumatol Arthrosc 15: 756-757. [Crossref]
- Michos J, Rallis J, Fassoulas A (2006) Fracture of femoral component in a resurfacing total knee arthroplasty. J Arthroplasty 21: 1068-1071. [Crossref]
- Saito S, Tokuhashi Y, Ishii T, Mori S, Hosaka K et al. (2011) Bilateral fatigue fracture of the femoral components in a cruciate-retaining cementless total knee prosthesis. Orthopedics 34: e688-e691. [Crossref]
- Sarraf KM, Wharton R, Abdul Jabar HB, Shah G, Singer GC (2013) Fatigue fractures of total knee prostheses: a cause of knee pain. Bull Hosp Jt Dis 72: 242-246. [Crossref]
- Swamy GN, Quah C, Bagouri E, Badhe NP (2014) Nontraumatic fracture of the femoral condylar prosthesis in a total knee arthroplasty leading to mechanical failure. Case Rep Orthop 2014: 896348. [Crossref]
- Swarts E, Miller SJ, Keogh CV, Lim G, Beaver RJ (2001) Fractured Whiteside Ortholoc II knee components. J Arthroplasty 16: 927-934. [Crossref]
- Wada M, Imura S, Bo A, Baba H, Miyazaki T (1997) Stress fracture of the femoral component in total knee replacement: a report of 3 cases. Int Orthop 21: 54-55. [Crossref]
- Whiteside LA, Fosco DR, Brooks JG Jr (1993) Fracture of the femoral component in cementless total knee arthroplasty. Clin Orthop Relat Res (286): 71-77. [Crossref]
- Vertullo CJ, Zbrojkiewicz D, Vizesi F, Walsh WR (2016) Thermal Analysis of the Tibial Cement Interface with Modern Cementing Technique. Open Orthop J 10: 19-25. [Crossref]