Dupuytren’s Disease in a Young Man of Sudanese Origin
A B S T R A C T
Background: Dupuytren’s disease (DD) may be more common in patients of African descent than previously thought.
Case Presentation: A 27-years-old gentleman of Sudanese origin presented with a 3-months history of a painful swelling in his right palm. An MRI scan showed no signs of malignancy, and an excision biopsy showed no signs of infection, including tuberculosis. Histology showed superficial fibromatosis or Dupuytren’s disease.
Conclusion: Our patient is very young to have developed DD, but studies of patients of African descent have not considered recurrence rate. It would be useful to investigate if the risk factors for recurrence are the same as those in patients of European descent, to be able to counsel them appropriately for surgery. Furthermore, there are no studies of the genetic variation underlying DD in an African population, to see if the genetic predisposing factors are the same as those identified in patients of European descent.
Keywords
Dupuytren’s disease, Africa, genetics, prevalence, Sudan
Background
Dupuytren’s disease (DD) is a progressive fibroproliferative disease of the palmar fascia with a prevalence of 5-25% of people in populations of European descent [1]. It had previously been thought to be rarer in Africa, with only sporadic case reports in the literature [1]. However, more recent studies have reported retrospective reviews of 75 patients treated in Ethiopia and 48 patients of African descent who underwent surgery for DD in South Africa [2, 3]. Therefore, DD may be more common in Africa than previously thought.
Case Presentation
A 27-years-old gentleman of Sudanese origin presented with a 3 months history of a painful swelling in his right hand. He had no history of trauma but on examination had a mass in the palm in line with his little finger (Figure 1). An MRI scan showed no signs of malignancy (Figure 2), so an excision biopsy was proposed. Microbiology samples showed no acid-fast bacilli and no bacteria or fungi were cultured. Histology showed superficial fibromatosis or Dupuytren’s disease.
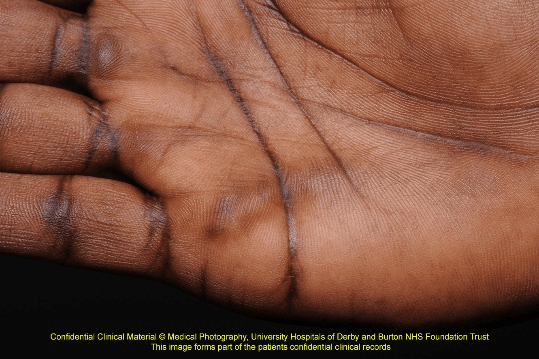
Figure 1: Clinical photograph of palmar mass.
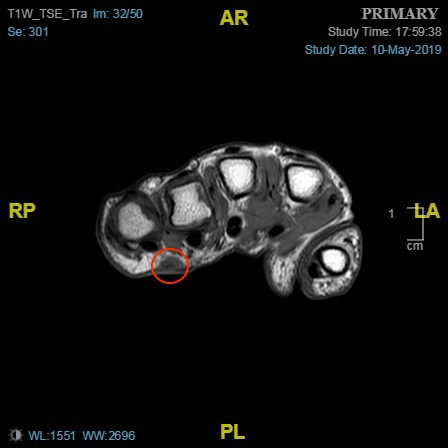
Figure 2: MRI of palmar lump.
Conclusion
Our patient is very young to have developed Dupuytren’s contracture. Studies in patients of European descent have identified risk factors for recurrence after surgery, including onset under 50 years, bilateral disease, ectopic disease (Ledderhose disease), first ray involvement, multiple ray involvement, family history and male gender [4]. While a study of 75 patients treated in Ethiopia found a broadly similar characteristics in terms of age at presentation and involvement of little and ring fingers, they did not consider recurrence rates [2]. It would be useful to study patients of African descent with DD to see if these risk factors are the same as those in patients of European descent, to be able to counsel them appropriately for surgery.
DD has a substantial heritable component, with 26 susceptibility loci identified in Genome-wide Association Studies of more than 8000 British, Dutch and German patients with Dupuytren’s disease [5]. There are currently no studies of the genetic variation underlying DD in an African population, and it would be interesting to see if the genetic predisposing factors are the same as those identified in patients of European descent.
Consent for Publication
Our patient gave written consent agreeing for his case, including photographs and investigations, to be reproduced in a journal.
Conflicts of Interest
None.
Funding
None.
Article Info
Article Type
Case ReportPublication history
Received: Tue 26, May 2020Accepted: Wed 10, Jun 2020
Published: Thu 25, Jun 2020
Copyright
© 2023 Julia Blackburn. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.GSCR.2020.01.02
Figures & Tables
References
- Sandip Hindocha, Duncan Angus McGrouther, Ardeshir Bayat (2009) Epidemiological evaluation of Dupuytren's disease incidence and prevalence rates in relation to etiology. Hand (N Y) 4: 256-269. [Crossref]
- A Gebereegziabher, A Baraki, Y Kebede, I Mohammed, V Finsen (2017) Dupuytren's contracture in Ethiopia. J Hand Surg Eur Vol 42: 26-28. [Crossref]
- Sefeane T, Mwangi P (2017) Incidence of Dupuytren’s disease in Africans: A report of 48 new cases and a literature review. S A Orthop J 16: 50-53.
- Ilse Degreef, Luc De Smet (2011) Risk factors in Dupuytren’s diathesis: is recurrence after surgery predictable? Acta Orthop Belg 77: 27-32. [Crossref]
- Michael Ng, Dipti Thakkar, Lorraine Southam, Paul Werker, Roel Ophoff et al. (2017) A Genome-wide Association Study of Dupuytren Disease Reveals 17 Additional Variants Implicated in Fibrosis. Am J Hum Genet 101: 417-427. [Crossref]