Comparison of Two Protocols for the Treatment of Class 2 Malocclusion
A B S T R A C T
Purpose: The purpose of this study was to compare the outcomes of the treatment with the twin block and modified twin block appliances in growing patients with Class 2 malocclusion.
Materials and Methods: A cephalometric analysis was performed in 51 patients. The twin block sample consisted of 23 patients, 10-girls and 13-boys (mean age 10.46±0.71 years at the start of treatment, T1, and 12.84±0.78 years at the end of active treatment, T2). The modified twin block sample consisted of 28 patients, 18 girls and 15 boys (mean age 11.78±0.91 years at T1, and 13.32±0.56 years at T2). The twin block activators were used during the day, except for eating time, and the modified ones were used only at night. Duration of the treatment was 16-20 months. The changes from T2 to T1 and the differences between the groups were compared with the analysis of variance.
Results: SNB angle in the twin block group showed 1.25±1.39 degrees change and in the modified twin block group, it exhibited 3.69±1.01 degrees change. Overjet in the group with twin block decreased 4.58±1.59 mm, and in the group with modified twin block it decreased 4.43±1.41 mm. In the modified twin block group, there was more retrusion of upper incisors in comparison with the twin block group. Accordingly, under the effect of modified twin block, retrusion of the upper lip was observed.
Conclusion: Through modifying the twin block appliance, it is possible to ensure the comfort of the patients by reducing the daily usage, to reposition the mandibula forward and to correct overjet and sagittal dento-skeletal relationships without increasing facial height and to improve positions of upper incisors and lips.
Keywords
Distal bite, class 2, twin blocks, modified twin block
Introduction
Distal bite malocclusion is one of the most common orthodontic problems, affecting approximately 10% of the population. It has been reported that this malocclusion accounts for 20-30% of all orthodontic patients. Skeletal distal bite can be caused by maxillary protrusion, mandibular retrusion, or a combination of both. As craniofacial structure, maxillo-mandibular relation, soft tissue thickness, tension of masticatory and facial muscles change because of distal malocclusions, aesthetics, pronunciation and chewing disfunction occurs, and 75% of the distal bite patients exhibit a retrusive chin position [1, 2].
The decision as to which is the most effective method to use in the treatment of growing patients with distal bite malocclusions has long been the source of considerable debate in the orthodontic literature. The most commonly used methods for distal bite treatments are tooth extraction, orthopaedic force effects with Headgears, functional jaw orthopaedics with functional appliances and molar distalization with different anchoring techniques. The goal of orthodontic treatment is to restore functions and aesthetics. For this purpose, it is necessary to create an individual balance between skeletal and soft tissues [3, 4]. In the treatment of distal malocclusions, as a result of forward repositioning of the mandible, tension in the intraarticular ligaments and adaptive changes in the articular cartilage occur thus accelerating the growth of the mandible [5-8].
The fixed orthodontic appliances for the forward repositioning of the mandible are also widely used in practice. It has been reported that fixed appliances have a positive effect on treatment of the distal bite malocclusions [9-11]. The twin block appliance is the most popular functional appliance, and it was first introduced by Clark in 1988. The appliance consists of upper and lower removable plates with acrylic blocks trimmed to an angle of 70 degrees. These separate the monoblock appliance into two parts ensuring the patient’s comfort [12]. Increase in the length of the mandible with the effect of the twin block appliance have been reported previously. It has been confirmed in the previous studies that as a result of changes in skeletal tissue with orthodontic treatment, adaptive changes occur in soft tissues [13-19].
The aim of this study was to compare the outcomes of the treatment with the twin block and modified twin block appliances in growing patients with distal bite malocclusions.
Materials and Methods
A cephalometric analysis was performed in 51 patients. The twin block sample consisted of 23 patient, 10-girls and 13-boys (mean age 10.46±0.71 years at the start of treatment, T1, and 12.84±0.78 years at the end of active treatment, T2). The modified twin block sample consisted of 28 patients, 18 girls and 15 boys (mean age 11.78±0.91 years at T1, and 13.32±0.56 years at T2). Duration of the treatment was 16-20 months. In order to evaluate changes in the stomatognathic system, lateral cephalograms were taken before treatment (T1) and after treatment (T2). The cephalograms were taken in a natural head position. The patients with temporomandibular joint pathology were not involved in the research.
In the group 1, Clark’s twin block appliance was used with upper expansion screw. The vertical activation was achieved by increasing the FWS by 2mm. Removable plates with acrylic blocks trimmed to an angle of 70 degrees. Following achievement of class I molar relationship, transition from the active to the stabilization phase was initiated. At this stage, a Hawley appliance with an inclined plane in the anterior region was used. In the 2nd group, a modified twin block appliance was used. The main difference between the conventional and the modified twin block appliances is that modified twin block appliance have inclined planes prepared in the form of backward 60˚ angle (Figure 1). The purpose of this is to prevent the backward movement of mandible.
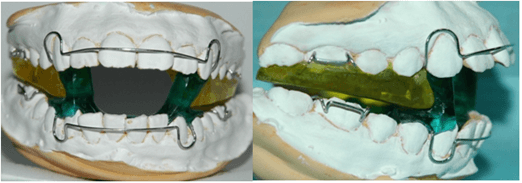
Figure 1: Modified twin block: frontal and side views.
During treatment with this appliance, patient moves the mandibula beyond the obligatory occlusion to open the mouth. The adjusting of occlusion is defined 3-4 mm behind the maximum anterior position of the mandibula, with 4-5mm of opening between upper and lower molars. To prepare this appliance, there is no need to determine the FWS and take into consideration the height. Because contact of the backward acrylic ledges on the top appliance and forward acrylic ledges on the bottom appliance prevents the backward mandibular movement. In severe distal bite malocclusions, for additional activation, 60˚ incline of the appliance is increased to 90˚. This change causes more forward position of the mandibula. The conventional twin block appliance was used for 24 hours per day, except during meals, and the modified one was used only at night. 37 linear and angular measurements were performed on the cephalograms, and they were calculated using the PORDIOS programme. The changes from T2 to T1 and the differences between the groups were compared with the analysis of variance.
Results
According to the results of the analysis, in the conventional twin block appliance group; S-N distance showed 1.15±0.56 mm of change and in the modified twin block group it showed 2.34±1.10 mm of change, both changes were statistically significant (p<0.001). Changes in ANS-PNS distance was 0.93±1.94 mm in the twin block group and 2.66±1.07 mm in the modified twin block group (Tables 1 & 2). According to the A-N perpendicular to FH parameter, sagittal development of maxilla was restricted in both groups. Judging by the change in the SNB angle, the forward movement of mandible was 1.25±1.39 degrees in the twin block group and in the modified twin block group it was 3.69±1.01. Vertically, with the effect of twin block appliance there was an increase in SN/GoGn by 0.13±1.59 and in ML/FH by 0.31±2.32 degrees, and with the effect of the modified appliance the increase was 1.96±2.02 and 1.41±2.61 degrees respectively.
Table 1: Cephalometric parameters in the twin block group.
|
Parameters |
T1 |
T2 |
T2-T1 |
p |
|
M±σ |
M±σ |
M±σ |
||
|
S-N |
70,49±3,09 |
71,64±3,09 |
1,15±0,56 |
*** |
|
ANS-PNS |
58,41±3,64 |
59,34±4,70 |
0,93±1,94 |
* |
|
SNA |
82,43±3,19 |
82,14±3,23 |
-0,29±1,02 |
|
|
A-N perp FH |
0,58±2,13 |
0,62±1,92 |
0,04±1,09 |
|
|
Pg-N perp FH
|
-6,88±3,35 |
-1,88±4,05 |
5,00±1,42 |
*** |
|
Co-Gn |
110,00±8,40 |
115,70±9,33 |
5,70±2,49 |
*** |
|
Go-Me |
67,92±10,78 |
70,54±12,20 |
2,62±2,12 |
*** |
|
SNB |
75,54±3,15 |
76,79±3,24 |
1,25±1,39 |
** |
|
SN/GoGn |
33,66±3,93 |
33,79±3,77 |
0,13±1,59 |
|
|
Gonial angle |
123,46±3,18 |
125,54±3,40 |
2,08±2,62 |
|
|
ML/FH |
23,71±3,71 |
24,02±4,45 |
0,31±2,32 |
|
|
SArGo |
137,21±5,80 |
138,46±4,53 |
1,25±4,25 |
|
|
WITS |
6,35±2,76 |
2,33±2,23 |
-3,99±1,29 |
*** |
|
Co-A |
89,19±5,43 |
91,02±6,29 |
1,82±2,44 |
** |
|
Max-Mand diff. |
20,83±5,91 |
24,68±5,57 |
3,85±2,04 |
*** |
|
ANB |
6,45±2,13 |
4,99±2,30 |
-1,46±1,01 |
*** |
|
PL/ML |
24,88±4,78 |
23,77±4,74 |
-1,11±1,81 |
|
|
Up. inc.-NA angle
|
24,50±5,33 |
20,46±4,75 |
-4,04±3,16 |
*** |
|
Up. inc.-NA distance |
5,60±1,44 |
3,88±1,46 |
-1,72±1,06 |
*** |
|
Low. inc.-NB angle |
20,55±5,68 |
22,19±6,81 |
1,65±1,80 |
|
|
Low. inc.-NB distance |
4,09±1,35 |
5,39±1,02 |
1,30±1,15 |
*** |
|
Pg-NB distance |
3,02±1,04 |
3,86±1,26 |
0,84±0,68 |
*** |
|
Holdaway |
1,07±2,01 |
1,37±1,70 |
0,30±1,60 |
|
|
Overjet |
8,36±1,63 |
3,78±0,75 |
-4,58±1,59 |
*** |
|
Overbite |
4,46±1,98 |
2,31±1,41 |
-2,15±1,72 |
** |
|
Okl/SN |
15,05±3,41 |
18,04±4,39 |
2,99±1,99 |
*** |
|
Alt k/ML |
97,11±6,40 |
96,98±6,28 |
-0,13±5,04 |
|
|
Inter-incisal |
118,42±6,96 |
129,72±7,22 |
11,30±7,89 |
*** |
|
N-ANS |
55,33±4,16 |
55,75±3,84 |
1,39±1,35 |
** |
|
ANS-Me |
64,41±6,28 |
67,46±7,21 |
3,05±1,41 |
*** |
|
N-Me |
115,26±8,97 |
119,76±9,48 |
4,5±1,66 |
*** |
|
S-Go |
73,28±6,79 |
76,44±6,89 |
3,16±1,53 |
*** |
|
Upper lip-E distance |
0,62±2,49 |
0,75±1,43 |
0,13±2,10 |
|
|
Lower lip-E distance |
0,89±2,52 |
0,75±1,47 |
-0,14±2,19 |
|
|
Interlabiale |
2,37±2,82 |
0,06±0,05 |
-2,31±2,82 |
** |
|
Nasolabial angle |
126,08±8,70 |
131,50±8,95 |
5,42±5,80 |
** |
|
Labiomental angle |
127,27±14,13 |
142,90±13,11 |
15,63±12,72 |
*** |
T1: before treatment; T2: after treatment.
*: p<0,05;
**: p<0,01; ***: p<0,001.
Table 2: Cephalometric parameters in the modified twin block group.
|
Parameters |
T1 |
T2 |
T2-T1 |
p |
|
M±σ |
M±σ |
M±σ |
||
|
S-N |
62,44±2,83 |
64,78±2,56 |
2,34±1,10 |
*** |
|
ANS-PNS |
52,38±4,99 |
55,04±5,31 |
2,66±1,07 |
*** |
|
SNA |
82,68±2,31 |
83,67±2,92 |
1,00±1,21 |
** |
|
A-N
perp FH |
0,42±2,44 |
0,68±2,28 |
0,27±1,16 |
|
|
Pg-N
perp FH |
-10,27±2,62 |
-6,68±2,97 |
3,59±1,57 |
*** |
|
Co-Gn |
93,10±4,09 |
96,67±4,87 |
3,57±1,77 |
*** |
|
Go-Me |
56,43±4,18 |
60,06±3,96 |
3,63±1,48 |
*** |
|
SNB |
75,41±2,79 |
79,10±2,46 |
3,69±1,01 |
*** |
|
SN/GoGn |
33,51±4,82 |
35,47±5,23 |
1,96±2,02 |
** |
|
Gonial
angle |
132,73±8,67 |
134,46±9,76 |
1,73±1,89 |
** |
|
ML/FH |
23,98±4,42 |
25,39±4,28 |
1,41±2,61 |
* |
|
SArGo |
137,86±12,06 |
138,18±9,73 |
0,33±3,80 |
|
|
WITS |
5,33±0,74 |
2,43±0,69 |
-2,89±0,80 |
*** |
|
Co-A |
77,69±4,35 |
78,45±4,88 |
0,76±1,99 |
|
|
Max-Mand
diff. |
16,26±2,96 |
19,07±4,43 |
2,81±2,72 |
*** |
|
ANB |
7,25±2,00 |
4,39±1,85 |
-2,87±0,89 |
*** |
|
PL/ML |
24,64±4,70 |
24,75±4,69 |
0,11±1,85 |
|
|
Up.
inc.-NA angle |
31,35±3,27 |
24,09±4,71 |
-7,25±4,97 |
*** |
|
Up.
inc.-NA distance |
5,60±1,39 |
3,59±1,59 |
-2,00±1,73 |
*** |
|
Low.
inc.-NB angle |
29,03±5,85 |
33,98±5,93 |
4,95±3,41 |
*** |
|
Low.
inc.-NB distance |
4,57±1,50 |
6,03±1,53 |
1,46±1,39 |
*** |
|
Pg-NB
distance |
2,58±1,63 |
1,93±1,73 |
-0,64±1,36 |
|
|
Holdaway
|
2,11±2,31 |
3,83±1,84 |
1,72±1,23 |
*** |
|
Overjet |
7,68±1,54 |
3,26±0,84 |
-4,43±1,41 |
*** |
|
Overbite |
5,01±0,96 |
3,75±0,71 |
-1,26±0,93 |
*** |
|
Okl/SN |
14,56±3,28 |
16,19±3,93 |
1,63±2,19 |
** |
|
Alt
k/ML |
94,96±4,81 |
98,99±5,52 |
4,04±1,68 |
*** |
|
Inter-incisal |
121,22±14,45 |
124,22±10,99 |
3,01±7,43 |
|
|
N-ANS |
49,66±7,27 |
52,84±7,36 |
3,18±0,96 |
*** |
|
ANS-Me |
55,46±3,20 |
57,87±4,00 |
2,41±2,50 |
** |
|
N-Me |
103,81±6,39 |
109,08±6,98 |
5,27±1,20 |
*** |
|
S-Go |
71,34±5,64 |
76,24±6,25 |
4,90±1,83 |
*** |
|
Upper
lip-E distance |
1,64±1,55 |
0,19±2,42 |
-1,45±1,80 |
** |
|
Lower
lip-E distance |
0,71±1,65 |
-0,38±3,07 |
-1,09±2,25 |
|
|
Interlabiale |
1,71±2,05 |
0,18±0,05 |
-1,53±2,05 |
** |
|
Nasolabial
angle |
121,33±9,45 |
122,88±7,55 |
1,56±6,68 |
|
|
Labiomental
angle |
121,44±7,66 |
135,47±9,64 |
14,03±13,15 |
*** |
T1: before treatment; T2: after treatment.
*: p<0,05;
**: p<0,01; ***: p<0,001.
According to the Wits appraisal measurement sagittal relationship between maxilla and mandible was corrected by 3.99±1.29 mm with the twin block and by 2.89±0.80 mm with modified twin block. In the twin block group ANB angle was 6.45±2.13 degrees before the treatment, with the effect of the original twin block it decreased by 1.46±1.01 degrees and was 4.99±2.30 degrees at the end of treatment. In the modified appliance group, at the beginning ANB was 7.25±2.00 degrees, then it decreased by 2.87±0.89 degrees and was 4.39±1.85 degrees at the end of the treatment. In the period of treatment with twin blocks, the angle of occlusal plane to SN increased by 2.99±1.99 degrees, in treatment with modified twin block it decreased by 1.63±2.19 degrees.
There was retrusion of upper incisors in both groups. In the modification group the level of retrusion was comparatively higher and intergroup difference was statistically significant (p<0.001). In the distal malocclusion treatment, overjet is one of the most focused measurements, thus, in the group with twin blocks it decreased by 4.58±1.59 mm. In the modified twin block group, overjet decreased by 4.43±1.41 mm. Comparison of the differences between groups is not statistically significant. In the twin block group overbite decreased by 2.15±1.72 mm, and in the modified twin block group it decreased by 1.26±0.93 mm.
Growth in lower 2/3 facial height (N-Me) and lower 1/3 facial height (ANS-Me) was similar between groups. Growth in middle 1/3 facial height (N-ANS) was greater in the modified twin block group (p<0.001). In the twin block group, a small amount of protrusion occurred at upper lip, but with the effect of the modified twin block 1.45±1.80 mm backward repositioning was observed (p<0.01).
Discussion
Treatment of skeletal distal bite malocclusion due to mandibular retrusion with functional appliances is a common treatment method in growing patients. This study was carried out to compare the changes made by twin block appliance and its modification to the stomatognathic system. According to the intergroup comparisons, twin block appliance was more effective at restricting growth of the maxilla (Table 3). In the group with modified twin blocks SNA angle showed that point A moved forward, and this was due to a change in SN plane. Studies have shown that activators restrict maxillary sagittal development [16, 20, 21].
Table 3: Comparison of the differences between the groups.
|
Parameters |
Twin block |
Modification |
p |
|
M±σ |
M±σ |
||
|
S-N |
1,15±0,56 |
2,34±1,10 |
*** |
|
ANS-PNS |
0,93±1,94 |
2,66±1,07 |
*** |
|
SNA |
-0,29±1,02 |
1,00±1,21 |
* |
|
A-N perp FH |
0,04±1,09 |
0,27±1,16 |
|
|
Pg-N perp FH
|
5,00±1,42 |
3,59±1,57 |
|
|
Co-Gn |
5,70±2,49 |
3,57±1,77 |
|
|
Go-Me |
2,62±2,12 |
3,63±1,48 |
|
|
SNB |
1,25±1,39 |
3,69±1,01 |
*** |
|
SN/GoGn |
0,13±1,59 |
1,96±2,02 |
|
|
Gonial angle |
2,08±2,62 |
1,73±1,89 |
|
|
ML/FH |
0,31±2,32 |
1,41±2,61 |
|
|
SArGo |
1,25±4,25 |
0,33±3,80 |
|
|
WITS |
-3,99±1,29 |
-2,89±0,80 |
|
|
Co-A |
1,82±2,44 |
0,76±1,99 |
|
|
Max-Mand diff. |
3,85±2,04 |
2,81±2,72 |
|
|
ANB |
-1,46±1,01 |
-2,87±0,89 |
*** |
|
PL/ML |
-1,11±1,81 |
0,11±1,85 |
|
|
Up. inc.-NA angle
|
-4,04±3,16 |
-7,25±4,97 |
*** |
|
Up. inc.-NA distance |
-1,72±1,06 |
-2,00±1,73 |
|
|
Low. inc.-NB angle |
1,65±1,80 |
4,95±3,41 |
|
|
Low. inc.-NB distance |
1,30±1,15 |
1,46±1,39 |
|
|
Pg-NB distance |
0,84±0,68 |
-0,64±1,36 |
*** |
|
Holdaway |
0,30±1,60 |
1,72±1,23 |
*** |
|
Overjet |
-4,58±1,59 |
-4,43±1,41 |
|
|
Overbite |
-2,15±1,72 |
-1,26±0,93 |
|
|
Okl/SN |
2,99±1,99 |
1,63±2,19 |
|
|
Alt k/ML |
-0,13±5,04 |
4,04±1,68 |
|
|
Inter-incisal |
11,30±7,89 |
3,01±7,43 |
|
|
N-ANS |
1,39±1,35 |
3,18±0,96 |
*** |
|
ANS-Me |
3,05±1,41 |
2,41±2,50 |
|
|
N-Me |
4,5±1,66 |
5,27±1,20 |
|
|
S-Go |
3,16±1,53 |
4,90±1,83 |
|
|
Upper lip-E distance |
0,13±2,10 |
-1,45±1,80 |
*** |
|
Lower lip-E distance |
-0,14±2,19 |
-1,09±2,25 |
|
|
Interlabiale |
-2,31±2,82 |
-1,53±2,05 |
|
|
Nasolabial angle |
5,42±5,80 |
1,56±6,68 |
|
|
Labiomental angle |
15,63±12,72 |
14,03±13,15 |
|
*: p<0,05;
**: p<0,01; ***: p<0,001.
According to the SNB angle, the modified twin block provided greater forward movement of the mandible. This outcome shows that reverse positioning of the inclined planes in the modified activators is effective in forward repositioning of the mandible. Although the SNB angle varied between groups, growth of mandibular length (Co-Gn) and mandibular corpus (Go-Me) was similar between the groups. Singh S and b. in their study showed that the length of the body of the mandible was no different from normal growth and development [22]. However, O’Brien et al. reported that the growth of the mandibula increased with the treatment effect [23]. Giuntini et al. reported both SNB and mandibular length increased with the twin block effect [21]. Changes in angles (GoGnSN, GoMeFH) were similar in two groups. This indicates that changing the form of the inclined plane has no effect on the vertical facial height.
According to the Wits measurement, the twin block and according to the ANB angle, modified twin block was more effective. The reason for such a difference, is the use of the occlusion line in the Wits measurement. The modified twin block based on this outcome, ensures stability of occlusal plane. Ehsani et al. in their studies, reported that the correction of the Wits was greater in twin block compared to Xbov group [16]. More retrusion in upper incisors shows that the modified appliance keeps the lower jaw forward more rigid and the backward force on the upper arch is higher. In both groups protrusion occurred at lower incisors. Statistically, the amount of protrusion at lower incisors between the groups was not significant. The protrusion in the lower incisors during the treatment with twin block have been reported previously. Van Der Plas et al. reported that the design of acrylic component of the activators did not change the incisor inclination [24]. By adjusting the height of the acrylic block created behind the inclined plane between the upper and lower part of the modified twin block, it is possible to control the dental vertical relationship. Changes in the lower lip, nasolabial, and labiomental angles were similar between the groups but, the upper lip repositioning was different. The upper lip retrusion caused by modification effect is a result of clinical manifestation of the forward mandibular movement.
Conclusion
Modifying the twin block appliance can ensure the forward movement of the mandible with reducing the daily usage. During the treatment with modified twin block appliance, it is possible to reposition the mandibula forward and to correct overjet and sagittal dento-skeletal relationships without increasing facial height and to improve protrusion of upper incisors and upper lips. The fact that patients do not use orthodontic appliances during the day ensures their comfort.
Article Info
Article Type
Research ArticlePublication history
Received: Mon 14, Jun 2021Accepted: Wed 18, Aug 2021
Published: Thu 23, Dec 2021
Copyright
© 2023 Gurel H.G.. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.DOBCR.2021.03.03
Figures & Tables
Table 1: Cephalometric parameters in the twin block group.
|
Parameters |
T1 |
T2 |
T2-T1 |
p |
|
M±σ |
M±σ |
M±σ |
||
|
S-N |
70,49±3,09 |
71,64±3,09 |
1,15±0,56 |
*** |
|
ANS-PNS |
58,41±3,64 |
59,34±4,70 |
0,93±1,94 |
* |
|
SNA |
82,43±3,19 |
82,14±3,23 |
-0,29±1,02 |
|
|
A-N perp FH |
0,58±2,13 |
0,62±1,92 |
0,04±1,09 |
|
|
Pg-N perp FH
|
-6,88±3,35 |
-1,88±4,05 |
5,00±1,42 |
*** |
|
Co-Gn |
110,00±8,40 |
115,70±9,33 |
5,70±2,49 |
*** |
|
Go-Me |
67,92±10,78 |
70,54±12,20 |
2,62±2,12 |
*** |
|
SNB |
75,54±3,15 |
76,79±3,24 |
1,25±1,39 |
** |
|
SN/GoGn |
33,66±3,93 |
33,79±3,77 |
0,13±1,59 |
|
|
Gonial angle |
123,46±3,18 |
125,54±3,40 |
2,08±2,62 |
|
|
ML/FH |
23,71±3,71 |
24,02±4,45 |
0,31±2,32 |
|
|
SArGo |
137,21±5,80 |
138,46±4,53 |
1,25±4,25 |
|
|
WITS |
6,35±2,76 |
2,33±2,23 |
-3,99±1,29 |
*** |
|
Co-A |
89,19±5,43 |
91,02±6,29 |
1,82±2,44 |
** |
|
Max-Mand diff. |
20,83±5,91 |
24,68±5,57 |
3,85±2,04 |
*** |
|
ANB |
6,45±2,13 |
4,99±2,30 |
-1,46±1,01 |
*** |
|
PL/ML |
24,88±4,78 |
23,77±4,74 |
-1,11±1,81 |
|
|
Up. inc.-NA angle
|
24,50±5,33 |
20,46±4,75 |
-4,04±3,16 |
*** |
|
Up. inc.-NA distance |
5,60±1,44 |
3,88±1,46 |
-1,72±1,06 |
*** |
|
Low. inc.-NB angle |
20,55±5,68 |
22,19±6,81 |
1,65±1,80 |
|
|
Low. inc.-NB distance |
4,09±1,35 |
5,39±1,02 |
1,30±1,15 |
*** |
|
Pg-NB distance |
3,02±1,04 |
3,86±1,26 |
0,84±0,68 |
*** |
|
Holdaway |
1,07±2,01 |
1,37±1,70 |
0,30±1,60 |
|
|
Overjet |
8,36±1,63 |
3,78±0,75 |
-4,58±1,59 |
*** |
|
Overbite |
4,46±1,98 |
2,31±1,41 |
-2,15±1,72 |
** |
|
Okl/SN |
15,05±3,41 |
18,04±4,39 |
2,99±1,99 |
*** |
|
Alt k/ML |
97,11±6,40 |
96,98±6,28 |
-0,13±5,04 |
|
|
Inter-incisal |
118,42±6,96 |
129,72±7,22 |
11,30±7,89 |
*** |
|
N-ANS |
55,33±4,16 |
55,75±3,84 |
1,39±1,35 |
** |
|
ANS-Me |
64,41±6,28 |
67,46±7,21 |
3,05±1,41 |
*** |
|
N-Me |
115,26±8,97 |
119,76±9,48 |
4,5±1,66 |
*** |
|
S-Go |
73,28±6,79 |
76,44±6,89 |
3,16±1,53 |
*** |
|
Upper lip-E distance |
0,62±2,49 |
0,75±1,43 |
0,13±2,10 |
|
|
Lower lip-E distance |
0,89±2,52 |
0,75±1,47 |
-0,14±2,19 |
|
|
Interlabiale |
2,37±2,82 |
0,06±0,05 |
-2,31±2,82 |
** |
|
Nasolabial angle |
126,08±8,70 |
131,50±8,95 |
5,42±5,80 |
** |
|
Labiomental angle |
127,27±14,13 |
142,90±13,11 |
15,63±12,72 |
*** |
T1: before treatment; T2: after treatment.
*: p<0,05;
**: p<0,01; ***: p<0,001.
Table 2: Cephalometric parameters in the modified twin block group.
|
Parameters |
T1 |
T2 |
T2-T1 |
p |
|
M±σ |
M±σ |
M±σ |
||
|
S-N |
62,44±2,83 |
64,78±2,56 |
2,34±1,10 |
*** |
|
ANS-PNS |
52,38±4,99 |
55,04±5,31 |
2,66±1,07 |
*** |
|
SNA |
82,68±2,31 |
83,67±2,92 |
1,00±1,21 |
** |
|
A-N
perp FH |
0,42±2,44 |
0,68±2,28 |
0,27±1,16 |
|
|
Pg-N
perp FH |
-10,27±2,62 |
-6,68±2,97 |
3,59±1,57 |
*** |
|
Co-Gn |
93,10±4,09 |
96,67±4,87 |
3,57±1,77 |
*** |
|
Go-Me |
56,43±4,18 |
60,06±3,96 |
3,63±1,48 |
*** |
|
SNB |
75,41±2,79 |
79,10±2,46 |
3,69±1,01 |
*** |
|
SN/GoGn |
33,51±4,82 |
35,47±5,23 |
1,96±2,02 |
** |
|
Gonial
angle |
132,73±8,67 |
134,46±9,76 |
1,73±1,89 |
** |
|
ML/FH |
23,98±4,42 |
25,39±4,28 |
1,41±2,61 |
* |
|
SArGo |
137,86±12,06 |
138,18±9,73 |
0,33±3,80 |
|
|
WITS |
5,33±0,74 |
2,43±0,69 |
-2,89±0,80 |
*** |
|
Co-A |
77,69±4,35 |
78,45±4,88 |
0,76±1,99 |
|
|
Max-Mand
diff. |
16,26±2,96 |
19,07±4,43 |
2,81±2,72 |
*** |
|
ANB |
7,25±2,00 |
4,39±1,85 |
-2,87±0,89 |
*** |
|
PL/ML |
24,64±4,70 |
24,75±4,69 |
0,11±1,85 |
|
|
Up.
inc.-NA angle |
31,35±3,27 |
24,09±4,71 |
-7,25±4,97 |
*** |
|
Up.
inc.-NA distance |
5,60±1,39 |
3,59±1,59 |
-2,00±1,73 |
*** |
|
Low.
inc.-NB angle |
29,03±5,85 |
33,98±5,93 |
4,95±3,41 |
*** |
|
Low.
inc.-NB distance |
4,57±1,50 |
6,03±1,53 |
1,46±1,39 |
*** |
|
Pg-NB
distance |
2,58±1,63 |
1,93±1,73 |
-0,64±1,36 |
|
|
Holdaway
|
2,11±2,31 |
3,83±1,84 |
1,72±1,23 |
*** |
|
Overjet |
7,68±1,54 |
3,26±0,84 |
-4,43±1,41 |
*** |
|
Overbite |
5,01±0,96 |
3,75±0,71 |
-1,26±0,93 |
*** |
|
Okl/SN |
14,56±3,28 |
16,19±3,93 |
1,63±2,19 |
** |
|
Alt
k/ML |
94,96±4,81 |
98,99±5,52 |
4,04±1,68 |
*** |
|
Inter-incisal |
121,22±14,45 |
124,22±10,99 |
3,01±7,43 |
|
|
N-ANS |
49,66±7,27 |
52,84±7,36 |
3,18±0,96 |
*** |
|
ANS-Me |
55,46±3,20 |
57,87±4,00 |
2,41±2,50 |
** |
|
N-Me |
103,81±6,39 |
109,08±6,98 |
5,27±1,20 |
*** |
|
S-Go |
71,34±5,64 |
76,24±6,25 |
4,90±1,83 |
*** |
|
Upper
lip-E distance |
1,64±1,55 |
0,19±2,42 |
-1,45±1,80 |
** |
|
Lower
lip-E distance |
0,71±1,65 |
-0,38±3,07 |
-1,09±2,25 |
|
|
Interlabiale |
1,71±2,05 |
0,18±0,05 |
-1,53±2,05 |
** |
|
Nasolabial
angle |
121,33±9,45 |
122,88±7,55 |
1,56±6,68 |
|
|
Labiomental
angle |
121,44±7,66 |
135,47±9,64 |
14,03±13,15 |
*** |
T1: before treatment; T2: after treatment.
*: p<0,05;
**: p<0,01; ***: p<0,001.
Table 3: Comparison of the differences between the groups.
|
Parameters |
Twin block |
Modification |
p |
|
M±σ |
M±σ |
||
|
S-N |
1,15±0,56 |
2,34±1,10 |
*** |
|
ANS-PNS |
0,93±1,94 |
2,66±1,07 |
*** |
|
SNA |
-0,29±1,02 |
1,00±1,21 |
* |
|
A-N perp FH |
0,04±1,09 |
0,27±1,16 |
|
|
Pg-N perp FH
|
5,00±1,42 |
3,59±1,57 |
|
|
Co-Gn |
5,70±2,49 |
3,57±1,77 |
|
|
Go-Me |
2,62±2,12 |
3,63±1,48 |
|
|
SNB |
1,25±1,39 |
3,69±1,01 |
*** |
|
SN/GoGn |
0,13±1,59 |
1,96±2,02 |
|
|
Gonial angle |
2,08±2,62 |
1,73±1,89 |
|
|
ML/FH |
0,31±2,32 |
1,41±2,61 |
|
|
SArGo |
1,25±4,25 |
0,33±3,80 |
|
|
WITS |
-3,99±1,29 |
-2,89±0,80 |
|
|
Co-A |
1,82±2,44 |
0,76±1,99 |
|
|
Max-Mand diff. |
3,85±2,04 |
2,81±2,72 |
|
|
ANB |
-1,46±1,01 |
-2,87±0,89 |
*** |
|
PL/ML |
-1,11±1,81 |
0,11±1,85 |
|
|
Up. inc.-NA angle
|
-4,04±3,16 |
-7,25±4,97 |
*** |
|
Up. inc.-NA distance |
-1,72±1,06 |
-2,00±1,73 |
|
|
Low. inc.-NB angle |
1,65±1,80 |
4,95±3,41 |
|
|
Low. inc.-NB distance |
1,30±1,15 |
1,46±1,39 |
|
|
Pg-NB distance |
0,84±0,68 |
-0,64±1,36 |
*** |
|
Holdaway |
0,30±1,60 |
1,72±1,23 |
*** |
|
Overjet |
-4,58±1,59 |
-4,43±1,41 |
|
|
Overbite |
-2,15±1,72 |
-1,26±0,93 |
|
|
Okl/SN |
2,99±1,99 |
1,63±2,19 |
|
|
Alt k/ML |
-0,13±5,04 |
4,04±1,68 |
|
|
Inter-incisal |
11,30±7,89 |
3,01±7,43 |
|
|
N-ANS |
1,39±1,35 |
3,18±0,96 |
*** |
|
ANS-Me |
3,05±1,41 |
2,41±2,50 |
|
|
N-Me |
4,5±1,66 |
5,27±1,20 |
|
|
S-Go |
3,16±1,53 |
4,90±1,83 |
|
|
Upper lip-E distance |
0,13±2,10 |
-1,45±1,80 |
*** |
|
Lower lip-E distance |
-0,14±2,19 |
-1,09±2,25 |
|
|
Interlabiale |
-2,31±2,82 |
-1,53±2,05 |
|
|
Nasolabial angle |
5,42±5,80 |
1,56±6,68 |
|
|
Labiomental angle |
15,63±12,72 |
14,03±13,15 |
|
*: p<0,05;
**: p<0,01; ***: p<0,001.
References
1.
Гараев ЗИ (2000) Генетические аспекты зубочелюстных аномалий и роль инбридинга
в их частоте и структуре. Автореф дис. д-ра мед.наук, М 39c.
2.
Buckhardt DR, McNamara
JA Jr, Baccetti T
(2003) Maxillary molar distalization or mandibular enhancement: a cephalometric
comparison of comprehensive orthodontic treatment including the pendulum and the
Herbst appliances. Am J Orthod Dentofacial Orthop 123:
108-116. [Crossref]
3.
Ahn HW, Chang YJ, Kim KA,
Joo SH, Park YG
et al.
(2014) Measurement of three-dimensional perioral soft tissue changes
in dentoalveolar protrusion patients after orthodontic treatment using a structured
light scanner. Angle Orthod 84:
795-802. [Crossref]
4.
Новрузов ЗГ, Алиевa РК,
Оздилер ОЕ (2018) Цефалометрическая оценка влияния съемных функциональных аппаратов,
используемых при лечении дистального прикуса, на высоту лица. Стоматология 97: 44-47.
5.
Meikle MC (2007) Remodelling the dentofacial skeleton: the biological basis of
orthodontics and dentofacial orthopedics. J Dent Res 86:
12-24. [Crossref]
6.
McNamara JA Jr, Sigler LM, Franchi L, Guest SS, Baccetti T (2010) Changes in occlusal relationships in mixed dentition patients
treated with rapid maxillary expansion. A prospective clinical study. Angle Orthod 80:
230-238. [Crossref]
7.
Clark WJ (2015) Twin Block Functional Therapy Applications in Dentofacial Orthopaedics.
3rd edition. London, Jaypee Brothers Medical Ltd 90.
8.
de Mattos JM, Palomo JM,
de Oliveira Ruellas AC,
Cheib PL, Eliliwi M et al. (2017) Three-dimensional
positional assessment of glenoid fossae and mandibular condyles in patients with
Class II subdivision malocclusion. Angle Orthod 87: 847-854. [Crossref]
9.
Lorena V, Josґe FCH, Guilherme
J, Mayara PP, Rachelle SR et al. (2018) Class
II malocclusion treatment effects with Jones Jig and Distal Jet followed by fixed
appliances. Angle Orthod 88:
10-19. [Crossref]
10. Vinni A, Rekha S, Sonal C (2018) Comparative
evaluation of treatment effects between two fixed functional appliances for correction
of Class II malocclusion: A single-center, randomized controlled trial. Angle
Orthod
88: 259-266. [Crossref]
11. Reis RS, Henriques JF, Janson G, Sanches FS, Henriques RP et al.
(2019) Cephalometric Changes Produced by the Distal Jet and Pendulum
Appliances in Class II Malocclusion Treatment. J Contemp Dent Pract 20:
32-39. [Crossref]
12. Clark WJ
(1988) The twin block technique. A functional orthopedic appliance system.
Am J Orthod Dentofacial Orthop 93: 1-18.
[Crossref]
13. Luo Y, Fang G
(2005) Effect of Twin-block appliance in the treatment of Class II and
division I malocclusion: a cephalometric study in 12 patients. Shanghai Kou Qiang
Yi Xue
14: 90-93. [Crossref]
14. Carlos FM, Paul WM (2006) Cephalometric facial soft tissue changes with the twin block
appliance in class II division 1 malocclusion
patients.
A systematic
review. Angle Orthod 76: 876-881. [Crossref]
15. Новрузов ЗГ, Алиева РК, Гараев ЗИ, Кулиевa СК (2018) Влияние на стоматогнатическую
систему модифицированного аппарата твинблок, используемого при лечении дистального
прикуса. Казанский медицинский журнал 99: 426-432.
16. Ehsani S, Nebbe B, Normando D, Lagravere MO, Flores Mir C
(2015) Dental and skeletal changes in mild to moderate Class II malocclusions
treated by either a Twin-block or Xbow appliance followed by full fixed orthodontic
treatment. Angle Orthod 85:
997-1002. [Crossref]
17. Babaki AF, Kashani ASM, Mokhtari S (2017) A Cephalometric
Comparison of Twin Block and Bionator Appliances in Treatment of Class II Malocclusion.
J Clin Exp Dent 9: e107-e111.
[Crossref]
18. Pattanaik S, Puvvula N, Mohammad N (2018) Accelerating
Treatment of Skeletal Class II Malocclusion using Fixed Twin Block Appliances. Int
J Clin Pediatr Dent 11: 146-150. [Crossref]
19. Di Biase AT, Lucchesi L, Qureshi U, Lee RT (2019) Post-treatment cephalometric changes in adolescent patients with Class II malocclusion
treated using two different functional appliance systems for an extended time period:
a randomized clinical trial. Eur J Orthod 42: 135-143.
[Crossref]
20. Franchi L, Alvetro L, Giuntini V, Masucci C, Defraia E et al. (2011) Effectiveness of comprehensive fixed appliance treatment used
with the Forsus Fatigue Resistant Device in Class II patients. Angle Orthod 81:
678-683. [Crossref]
21. Giuntini V, Vangelisti A, Masucci C, Defraia E, Mcnamara JA et al. (2015) Treatment effects produced by the Twin-block appliance vs the
Forsus Fatigue Resistant Device in growing Class II patients. Angle Orthod 85:
784-789. [Crossref]
22. Singh S, Singh M, Saini A, Misra V, Sharma VP et al.
(2010) Timing of myofunctional appliance therapy. J Clin Pediatr
Dent
35: 233-240. [Crossref]
23. O’Brien K, Wright J, Conboy F, Sanjie YW, Mandall N et al. (2003) Effectiveness of treatment for Class II malocclusion with the Herbst or Twinblock appliances: a randomized, controlled trial. Am J Orthod Dentofacial Orthop 124: 128-137. [Crossref]
24. Van Der Plas Mc, Janssen Ki, Pandis N, Livas C (2017) Twin Block appliance with acrylic capping does not have a significant inhibitory effect on lower incisor proclination. Angle Orthod 87: 513-518. [Crossref]