Cell-Wall-Deficient Bacteria in Oral Biofilm: Association with Periodontitis
A B S T R A C T
Cell-wall-deficient bacteria are those that lack cell walls and live in a pleomorphic state. The genus Mycoplasma and L-form bacteria are both members of this group. The aim of this study was to search cell-wall-deficient bacteria in periodontal biofilm and link their presence to periodontal disease. Eighty-nine individuals were recruited and divided into three groups: periodontally healthy individuals, individuals with chronic periodontitis, and those with aggressive periodontitis. The presence of cell-wall-deficient bacteria was detected in freshly collected biofilm by light microscopy, transmission electron microscopy (TEM) with and without electron microscopy in situ hybridization, atomic force microscopy and DNA stain (Hoechst). A new dichotomic index of classification for prevalence and morphologic variants was developed to classify cell-wall-deficient bacteria in periodontal biofilm. Cell-wall-deficient bacteria were found in periodontal biofilm and classified into protoplastic, everted, filament and intracellular forms, the last one mainly associated with aggressive periodontitis. We also assessed the prevalence of periodontopathic bacteria by means of polymerase chain-reaction (PCR) and found no clear, statistically significant, correlation among periodontal pathogens tested (except T. denticola) that allowed individuals with chronic periodontitis to be distinguished from those with aggressive periodontitis. Association between cell-wall-deficient bacteria and periodontal condition was: periodontally healthy, 3.3% (1/30); individuals with chronic periodontitis, 30.6% (11/36); and those with aggressive periodontitis, 100% (23/23). Cell-wall-deficient bacteria were detected in periodontal biofilm and linked to aggressive periodontitis.
Keywords
Aggressive periodontitis, chronic periodontitis, phase contrast microscopy, atomic force microscopy, TEM, electron microscopy in situ hybridization, CWDB, L-forms, dental plaque, PCR
Introduction
Since the middle of the last century, there has been a rapid knowledge evolution in the field of microbiology that is reflected in a non-homogeneous literature. Analyzing mid-1900s studies on “non-classical” bacterial forms, we found terms such as ‘cell-wall-deficient bacteria’ (CWDB), ‘pleuropneumonia-like organisms (PPLO)’, ‘Mycoplasma’, ‘L-form bacteria’, ‘spheroplast’, and ‘protoplast’ used to describe pleomorphic forms of different bacteria.
Since the discovery of CWDB, several studies have linked their presence to different diseases, but their role remains unclear. Some authors believe that the ability of bacteria to lose the cell wall and to replicate in the CWD state represents a primordial reproduction mechanism [1]. We now know that the bacteria that can colonize the oral cavity belong to more than 700 species [2]. Some researchers have stated that probably all known bacterial species can be converted to CWDB by a variety of inducing agents such as cell-wall-inhibiting antibiotics and high concentrations of amino acids and enzymes [3, 4]. No studies are reported on oral CWDB.
Cell-wall-deficient bacteria (CWDB) are those that lack a cell wall, live in a pleomorphic state, and proliferate by a mechanism of membrane tubulation, blebbing, or vesiculation [1, 3]. The genus Mycoplasma and L-form bacteria are both members of this group. ‘Mycoplasma’ is the term now used to describe a heterogenic group of bacteria (members of mollicutes), of very small genome size, that have evolved from walled bacteria (members of firmicutes). The clinical picture of Mycoplasma infections in humans and animals is more suggestive of damage due to host immune and inflammatory responses rather than to direct toxic effects by Mycoplasmal cell components [5].
Mycoplasma salivarium (or the pleuropneumonia-like organism PPLO) was found in the oral cavities of all individuals with natural dentition and was absent in edentulous individuals [6]. M. salivarium can play an etiologic role in some oral infections, including periodontal diseases [7]. One study reported that the proportion of Mycoplasmas is related to periodontal disease severity [8]. Mycoplasmas have been detected in a patient diagnosed as having juvenile periodontitis [9]. L-form bacteria were described for the first time more than 80 years ago and can be differentiated into stable or unstable, depending on their ability to revert to the parental, cell-walled form [10, 11]. Recent reports hypothesized that early key steps in the evolutionary development of the bacterial domain of life have been achieved by CWD bacteria, and that the mechanism whereby bacteria can live without a cell wall may have been retained by modern cells as a back-up process for use when cell wall synthesis is compromised [1, 12]. Reversible model of transient cell wall-deficiency based on E. coli that allows studying transition, L-form reproduction and reversion in a controlled manner has been recently presented [13].
Some authors described the survival of E. coli L-forms under lethal stress, whether by autoclaving or boiling [14]. Since their identification, numerous reports have linked CWD bacteria with the persistence and recurrence of many diseases such as osteomyelitis, rheumatism, endocarditis, Alzheimer's disease, Lyme disease, and even cancer [4, 15-18]. Ultrastructure analysis has been used to identify Mycoplasma and L-forms of bacteria in cell culture [19, 20].
Periodontitis is a disease caused by lack of homeostasis between complex mixed-species periodontal biofilm and host multifactorial response. Periodontal disease manifestation varies from mild chronic to severe aggressive, depending on still-not-completely-understood predisposing factors. In a systematic review, the authors found no clear correlation among periodontal pathogens that allow individuals with chronic periodontitis (CP) to be distinguished from those with aggressive periodontitis (AP) [21]. In another study, the correlation among periodontal pathogens resulted in large differences in the composition of subgingival plaque between CP and AP [22].
Since literature associating CWD bacteria with periodontal disease is almost non-existent, we have attempted to verify the hypothesis that in chronic and aggressive forms of the disease, the relationship between periodontal biofilm and inflammatory host response is linked to the presence of CWD bacteria. The purpose of this study was to classify the different forms of CWDB present in periodontal biofilm and associate their presence with periodontal disease. We first assessed the prevalence of major periodontopathic bacteria, in our samples, by means of polymerase chain-reaction (PCR). We then developed a simple method to identify and classify CWD bacteria in freshly collected biofilm using phase-contrast microscopy and evaluated distribution of DNA in these microorganisms using Hoechst dye. The presence of CWDB in periodontal biofilm was also assessed after dissociated-biofilm culture.
In a previous study, we used atomic force microscopy (AFM) on oral biofilm to study morphological characteristics of some periodontal bacteria at high magnification with simple and conservative sample preparation [23]. In this study, we used AFM to identify morphological characteristics of CWDB. Finally, we confirmed the presence of CWDB in periodontal biofilm by transmission electron microscopy (TEM) with and without in situ hybridization.
Materials and Methods
I Study Population
Participants were diagnosed and then categorized into 3 clinical groups according to AAP periodontal classifications [22]. We set an age cut off point of 35 years and verify the presence of two or more interproximal, nonadjacent sites with attachment loss of ≥ 6 mm occurring at a minimum of two different teeth and accompanied by bleeding on probing for aggressive periodontitis as suggested in recent reviews [24, 25]. Eighty-nine individuals were randomly selected from among those referred to the periodontal and general dentistry department at the Fatebenefratelli “S. Giovanni Calibita” hospital in Rome, Italy, and were divided into groups as follows: 30 periodontally healthy (mean age, 51 yrs; age range, 25-68 yrs; males, 15; females, 15), 36 with chronic periodontitis (mean age, 57.2 yrs; age range, 36-75 yrs; males, 22; females, 14), and 23 with aggressive periodontitis (mean age, 31,8 yrs; age range, 24-35 yrs; males, 6; females, 17).
For each patient, the following data were recorded and used for classification: bleeding index, plaque index, probing depth, and clinical attachment level. Periodontal examination was carried out by a single trained and calibrated examiner (TD). Calibration of clinical periodontal parameters was carried out on five participants (k value 0.83). Individual data (PD, CAL, PI, BOP, etc.) for all patients are presented in the online Supporting Information (Table S1). Individuals were excluded if: they had fewer than 16 teeth, they had taken antibiotics in the preceding 3 months, they had received periodontal treatment in the preceding 6 months, they were smokers, or they had systemic conditions affecting their periodontal status according to AAP classifications.
Written informed consent was obtained from each patient. Examinations on patients and samples of oral biofilm were part of routine and diagnostic care and used for statistical purpose. All data was anonymized prior to analysis. The review board of the Ethics Committee at the Fatebenefratelli “S. Giovanni Calibita” hospital, in charge of preliminary research activity, was informed of the study, examined the documents, approved this consent procedure, and provide an oral waiver for the proposed protocol. However, the review board decided to not submit the proposed protocol to the Ethics Committee for a formal approval because sample and analysis on oral bacteria is considered normal clinical practice, it was believed that the issues did not meet those expressly covered by the rules.
II Microbiological Samples
Biofilm samples were collected, by means of a sterile curette, from the deepest pocket area of individuals with periodontitis after careful removal of supragingival plaque. Samples from individuals with periodontitis were pooled samples collected from the 4 deepest pockets, one per quadrant, and samples from periodontally healthy individuals were pooled samples collected from 4 first molars (or second molars if the first was missing), one per quadrant. The biofilms were dispersed in 200 μL of sterile saline solution (0.9%) by means of a sterile hypodermic syringe, and a 50 μL quantity of the pool obtained was applied to a glass slide and covered with a coverslip. Excess solution was removed from the edge of the coverslip, and the slide was sealed with nail varnish. Microbiological samples were analysed by two operators (GF, TD) blinded to the clinical status of the study participants. Both operators were trained to look for CWDB according to our classification, and frequency of agreement was 93% (k value 0.87). A microscopic image was obtained with an optical microscope in phase contrast at 200x, 400x, and 600x magnifications (BA310 LED Motic Asia, Hong Kong).
The images and movies were captured with a digital camera (Canon 7D). Two biofilm samples for each clinical group were also dispersed in Luria-Bertani broth (LB) containing 40 mM MgCl2, 1 M sucrose and 40 mM maleic acid pH 7 to test whether a higher level of osmotic protection allows better preservation of CWDB. Seven biofilm samples (2 from periodontally healthy individuals, 2 from chronic periodontitis individuals, 3 from aggressive periodontitis individuals) were processed for bacterial culture. Nine biofilm samples (3 from periodontally healthy individuals, 3 from chronic periodontitis individuals, 3 from aggressive periodontitis individuals) were processed for transmission electron microscopy (TEM) and electron microscopy in situ hybridization.
III PCR
Samples for PCR were collected from individuals with chronic and aggressive periodontitis and processed as previously described [26]. The amplified DNA was applied to the DNA-Strip® matrix to test the prevalence of periodontopathic bacteria (micro-IDent ® plus for A. actinomycetemcomitans, P. gingivalis, P. intermedia, T. forsythia, T. denticola, F. nucleatum, C. rectus, P. micra, E. nodatum, E. corrodens, and Capnocytophaga sp.; Hain Lifescience GmbH, Nehren, Germany).
IV TEM
Biofilm samples collected as reported above were fixed in Karnovsky’s solution (2% paraformaldehyde/2% glutaraldehyde) for 24h, embedded in 2% agarose and post-fixed in 2% osmium tetroxide. After washing with 0.1 M phosphate buffer, samples were dehydrated by a series of incubations in 30%, 50% and 70%, ethanol. Dehydration was continued by incubation steps in 95% ethanol, absolute ethanol, and propylene oxide, then samples were embedded in Epon (Agar Scientific, Stansted Essex CM24 8GF United Kingdom) [27]. After incubation at 60°C for 48h, epon embedded cells were cut by diamond knife (DiaTome, 1560 Industry, Hatfield, PA 19440). In detail, 60-80 nm ultrathin sections (silver-yellow colour) were collected onto cupper grids and staining with heavy metals solutions as previously described [28]. All samples were observed by TEM Hitachi FA 7100.
V Pre-Embedded Electron Microscopy in situ Hybridization
After fixation in Karnovsky’s solution small fragment of samples were treated for in situ Hybridization. Briefly, for bacterial permeabilization, samples were incubated with both lysozyme solution (Thermo Scientific, Waltham, MA USA) and Triton X-100 (Thermo Scientific, Waltham, MA USA) at room temperature for 1h. Then, samples were pre-treated with EDTA citrate Ph 7.8 (UCS Diagnostics, Rome, Italy) at 95°C for 20 min, and incubated with EUB 338 biotinylated probe (5’ GCT GCC TCC CGT AGG AGT 3’) (Eurofins Genomics, Ebersberg, Germany) for the detection of bacterial 16S rRNA in a humid chamber for 24h at 37°C. Once completed hybridization step, samples were washed in 50 ml of stringent washing buffer (Abbot, Illinois, U.S.A) at 37°C for 30 min. Whereupon, samples were incubated with streptavidin-gold nanoparticles (20nm) conjugated (Agar Scientific, Stansted Essex CM24 8GF United Kingdom) for 2h at room temperature. Finally, all samples were embedded in Epon and observed by TEM as described above.
VI Atomic Force Microscopy
Biofilm samples for atomic force microscopy were collected as previously described [23]. Images were taken with AFM SolverPro-M®, equipped with ETALON HA_NC/15 probes (NT-MDT, Moscow, Russia) in semi-contact and phase modes, and scanned per sample. All images were acquired at 1,024 lines. Image analysis was performed with the free software Gwyddion® (Link).
VII Fluorescence Staining
Hoechst 33342 (0.5 μg mL-1; Sigma-Aldrich, St. Louis, MO, USA) was added to 50 μL of six biofilm samples pool obtained from individuals with chronic periodontitis, aggressive periodontitis and from periodontally healthy individuals. Slides were mounted with Mowiol®, and fluorescent images were taken with a Zeiss Axioplan2 microscope.
VIII Bacterial Culture
Biofilm samples collected as reported above were transferred in a 15 ml sterile tube containing 5 ml of Luria-Bertani broth (LB) and incubated for 2 days at 30°C without shaking. Four milliliters of each culture were filtered using a sterile 0.45 μm filter (Sarstedt, Germany) to exclude walled bacteria and eukaryotic cells. To concentrate samples, filtered material was centrifuged and resuspended in 50 μl of LB to which 1 μl of Hoechst (stock solution 1 mg/ml) was added. Samples were spotted on a slide for microscopy analysis. Phase contrast and fluorescent images were taken with a Zeiss Axioplan2 microscope connected to a digital camera.
IX Index for CWDB Classification
The nature of CWD L-form bacteria, with no homogeneous distribution inside the biofilm, and their high polymorphism (intra- or extracellular and a large size range) prevented us from using traditional counting methods; therefore, we created a CWDB classification index based on descriptions present in the literature [29]. We identified 4 different morphological varieties of CWDB: protoplastic with or without inclusion, everted, filament, and intracellular forms.
Based on the quantity and quality of CWDB present, we developed a dichotomic index to assess their prevalence in periodontal biofilm:
i. Grade 0 (G0) was assigned when, in 10 random fields (100 x 100 microns), the absence of CWDB or the presence of only protoplastic form without granules < 1% of total bacteria was recorded; and
ii. Grade 1 (divided into high and low concentrations, G1L, G1H) was assigned when, in 10 random fields (100 x 100 microns), one of the following conditions was met:
a. G1L - when 2 kinds of CWDB were present, or one or more areas of the slide had CWDB prevalence > 5% or
b. G1H - when 3 or more kinds of CWDB were present, or one or more areas with high prevalence of CWDB were found (> 70%).
X Statistical Analysis
Differences in the prevalence of CWDB in healthy individuals and those with chronic or aggressive periodontitis were analysed by the chi-square test with Prism 6 GraphPad software. Cohen's kappa coefficient was used for calibration of clinical periodontal parameters and for index score agreement between operators.
Results
I Classifications of CWDB
By analysing the literature on the morphology of CWDB, L-form, and Mycoplasmas, we found that some bacterial forms in our samples matched the descriptions found in those studies. Based on these descriptions, we classified various types of CWD bacteria into the following forms and tested the prevalence of each form in our study population. The protoplastic form varies from tiny motile granules (< 1 μm) to large spheric formations (up to 30 μm). The spheric form is the most frequent and can contain vesicles or granules (motile or not) (Figures 1a, 2a, 2b & 2e-2h, Movies S1 & S2). Due to the plasticity of the cellular membrane, some forms appear elongated or ovoid. Figure 1b shows a high prevalence of spheric forms. Analysing videos of samples, we were able to capture the transformation of a spirochete-like in a protoplastic forms (Figures 3a-3c, Movie S8). We also used atomic force microscope (AFM) to examine CWDB at higher magnification, (Figure 3d) shows spirochete with spheric form of CWDB attached. Staining with Hoechst (Figures 3e-3j) indicated an inhomogeneous distribution of DNA as genetic material within larger L-form cells.
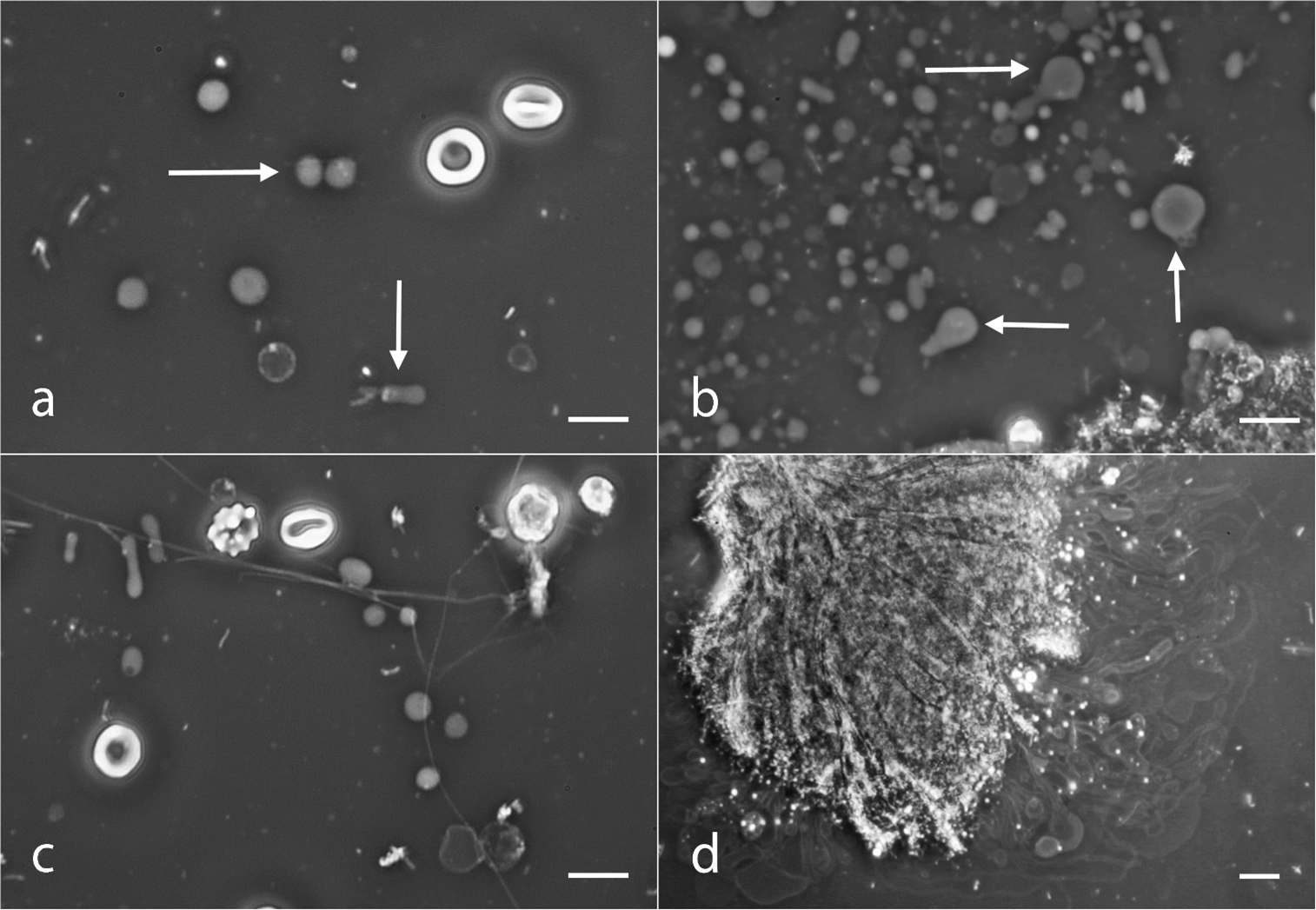
Figure 1: Protoplastic, everted, and filament forms of CWDB. a) Low prevalence of the protoplastic form, arrows indicate forms with motile granule inside. b) High prevalence of protoplastic tiny motile granules (< 1 μm) and large spheric formations (> 30 μm, see arrows). c) Filament-form long, tiny, branched formation connected with some protoplastic forms. d) Everted form with tubular and bubble formations emerging from plaque aggregate. Light microscope in phase contrast. Bar: 10 μm.
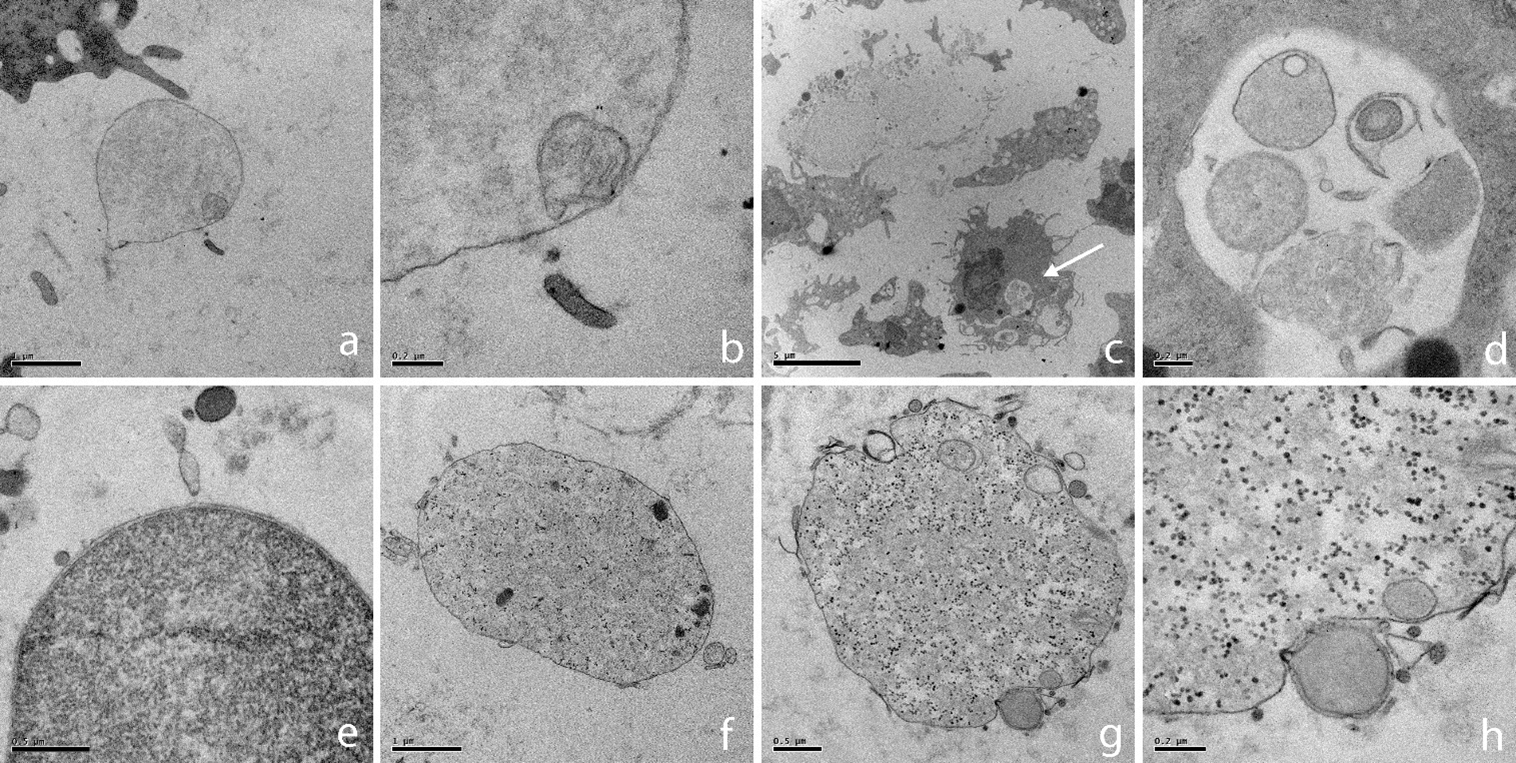
Figure 2: TEM images of CWDB from aggressive periodontitis individuals. a) CWDB with light granular cytoplasm and a small vesicle inside. 20000x. b) Vesicle at higher magnification, double layer membrane is easy visible. 80000x. c) A granulocyte containing a CWDB inside a vacuole (arrow); mag. 5000x. d) A higher magnification of the same vacuole shown in c. CWDB with lighter or darker cytoplasm can be observed inside the vacuole. 60000x. e) CWDB with dark granular cytoplasm and a well conserved plasma membrane. Light and dark small vesicles are present outside cell membrane. 50000x. f) Large CWDB (up to 5 μm) with ribosome-like granules and dark inclusions. 20000x. g) CWDB with ribosome-like granules. Light and dark small vesicles are present inside and outside cell membrane; 30000x. h) Magnification of previous image; 80000x.
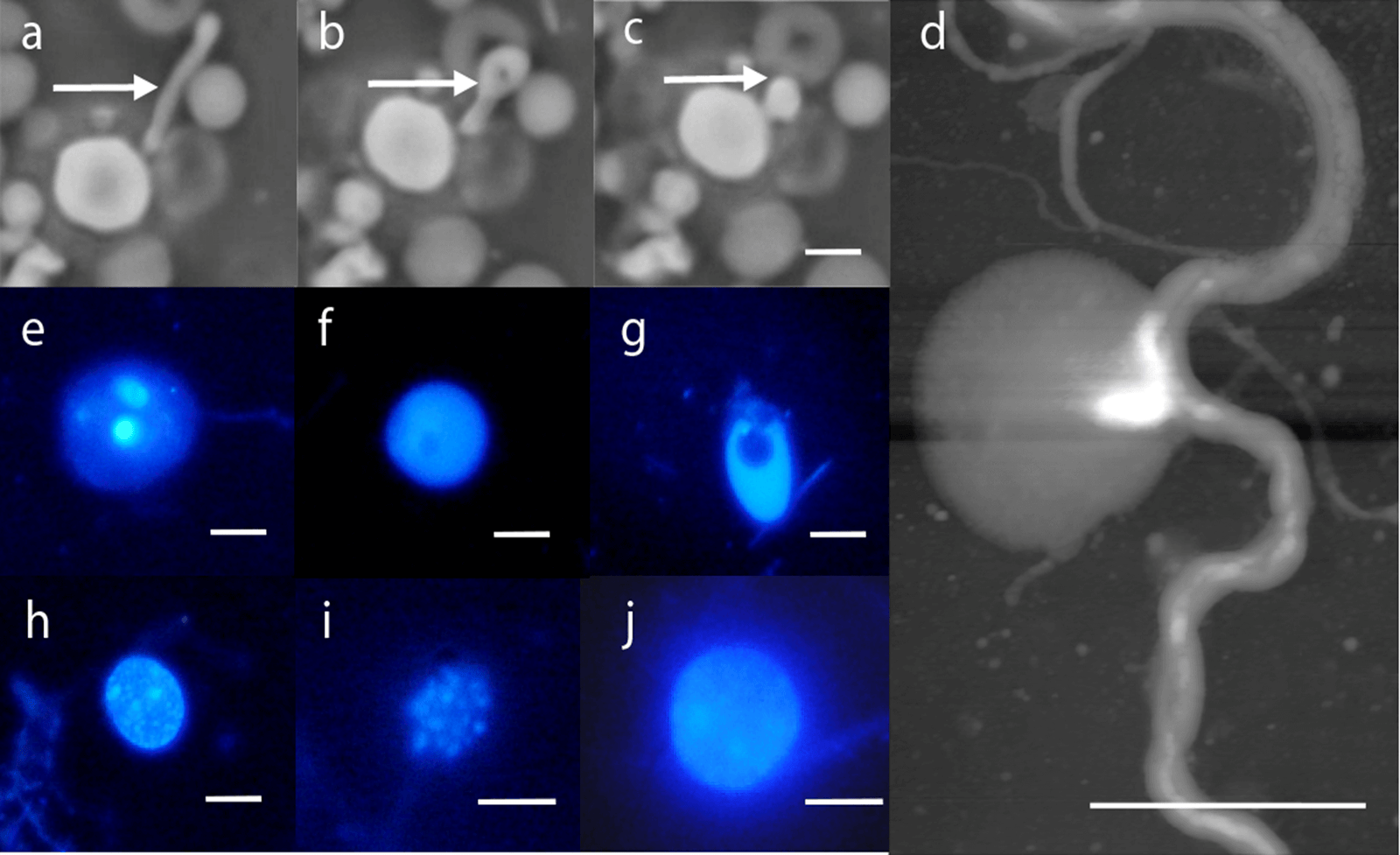
Figure 3: a-c) Time-lapse photography of the transformation of a spirochete-like bacteria in a spheric form of CWDB Light microscope in phase contrast. d) Spirochete with spheric form of CWDB attached. Atomic force microscopy. Image height is 0-140 nm. e-j) Hoechst immunofluorescence staining indicating small vesicles and inhomogeneous distribution of DNA. Bar: 10 μm.
Filament forms have the shape of long, tiny, non-motile formations (0.5-1 μm diameter, more than 100 μm long). Some of these are branched, connected with granulocytes or protoplastic forms (Figure 1c). Everted forms originate from the surfaces of bacterial aggregates and can be recognized by their long motile tubular or bubble form. Their size ranges from small, elongated bubbles (5 μm) to long tubular formations (5-10 μm diameter, more than 100 μm long). Some of these forms show motile granules inside the external membrane (Figure 1d, Movie S3).
The intracellular forms may be present in granulocytes, keratinocytes, and erythrocytes (Figure 4). CWDB present in leukocytes have the shape of tiny and highly motile granules. Invaded granulocytes have the tendency to die by necrosis and to release CWDB into the surrounding space (Figure 4b, Movie S4). CWDB present in keratinocytes have the shape of tiny and highly motile granules (Figure 4a, Movie S6). They are located in cytoplasmic space and can sometimes be found inside nuclear space (Figures 4d & 4e, Movie S5). CWDB were also seen attached to the surface of erythrocytes in the form of motile protrusions that have the shape of long pearl-like chains extending up to 30 μm from the cell (Figure 4c, Movie S7).
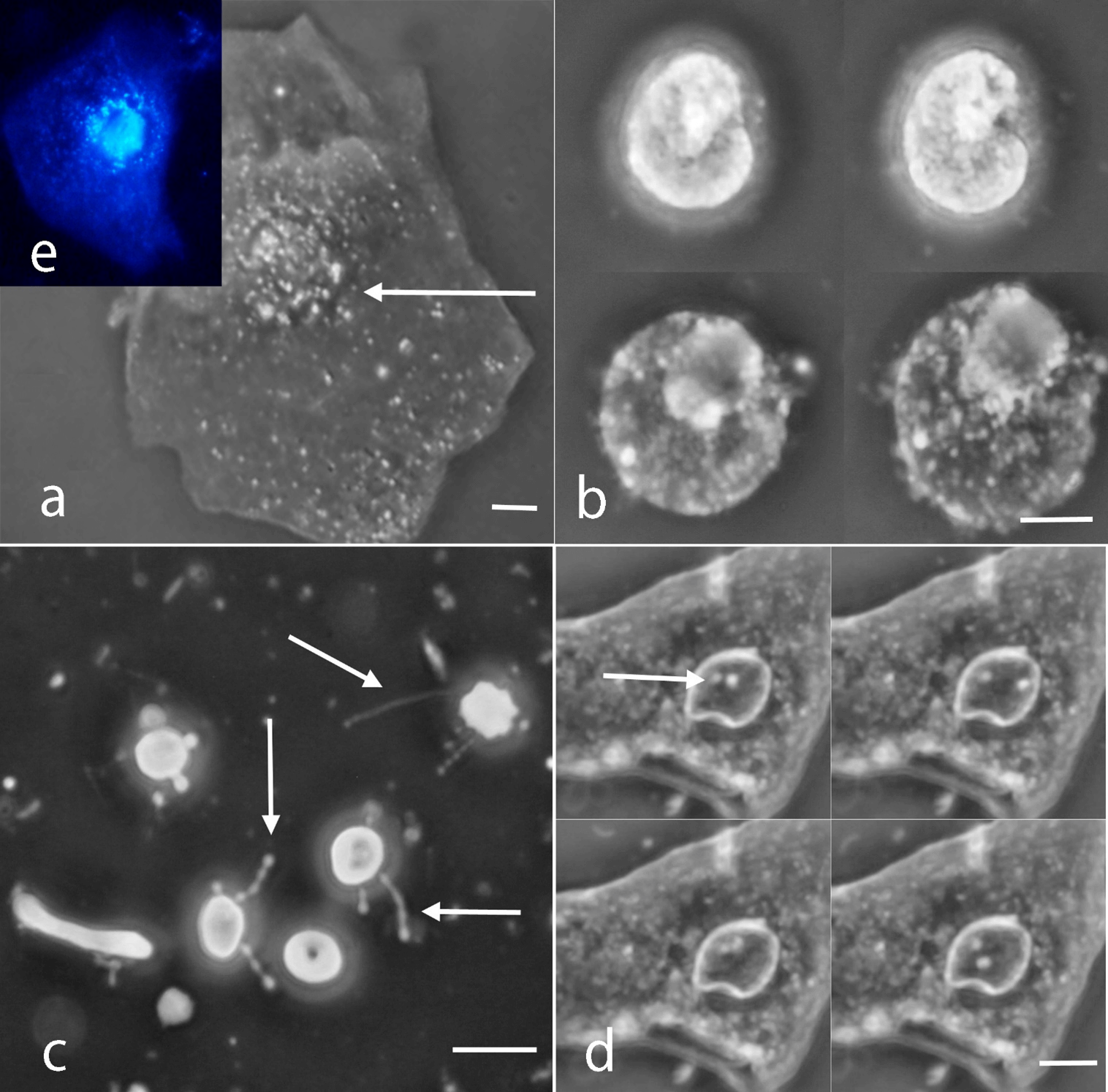
Figure 4: Intracellular form of CWDB. a) CWDB inside cytoplasmic space of a keratinocyte. Arrows indicate motile CWDB. b) Time-lapse photography of a granulocyte invaded by CWDB, releasing tiny forms of bacteria into the surrounding space. c) CWDB present in erythrocytes. Arrows indicate motile chain of CWDB. d) CWDB inside nuclear space of a keratinocyte. Arrows indicate motile CWDB. Light microscope in phase contrast. e) CWDB inside cytoplasmic space of a keratinocyte Hoechst immunofluorescence staining. Bar: 10 μm.
We also included images and videos of samples obtained from periodontally healthy individuals (Figures 5a & 5b) and chronic periodontitis (Figures 5c, 5d & 6a-6d, Movie S9) which do not contain CWDB bacteria but show only normal bacterial morphology. No differences were seen between biofilms dispersed in saline solution and in osmoprotective media.
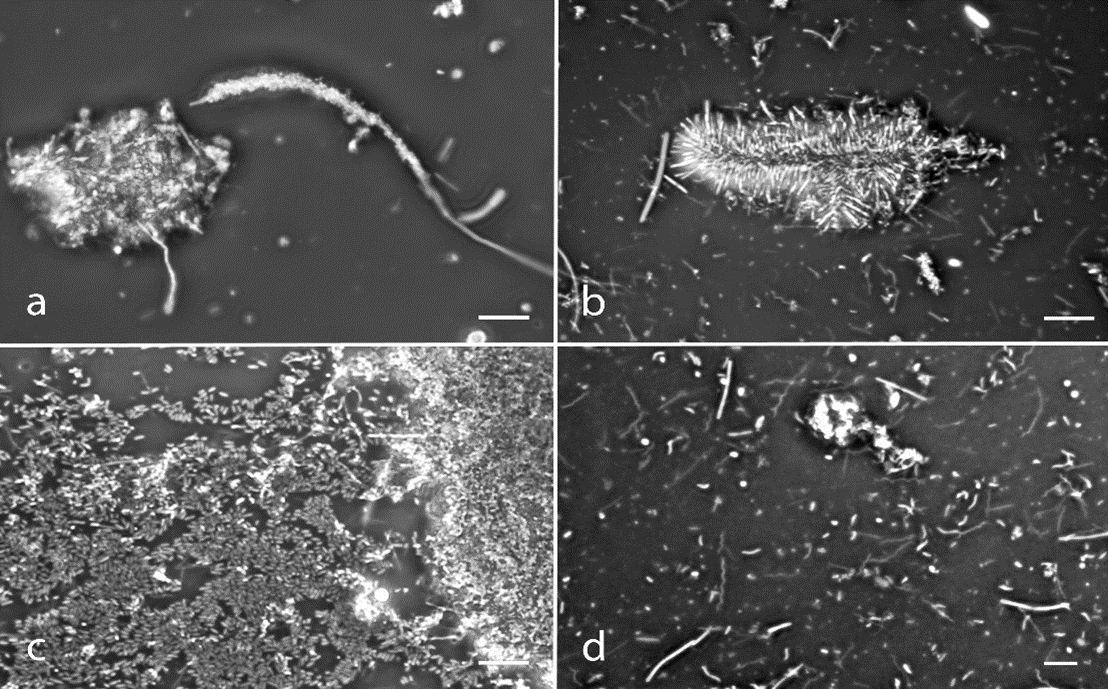
Figure 5: Control images with classical bacterial forms. Periodontally healthy individuals a) corncob formation, b) “test-tube brush” formation, c) coccoid and straight rod bacteria. Chronic periodontitis individuals d) all major morphological categories are represented (cocci, straight rods, filament, spirochete), a granulocyte is also present in the upper half. Bar = 10 μm.
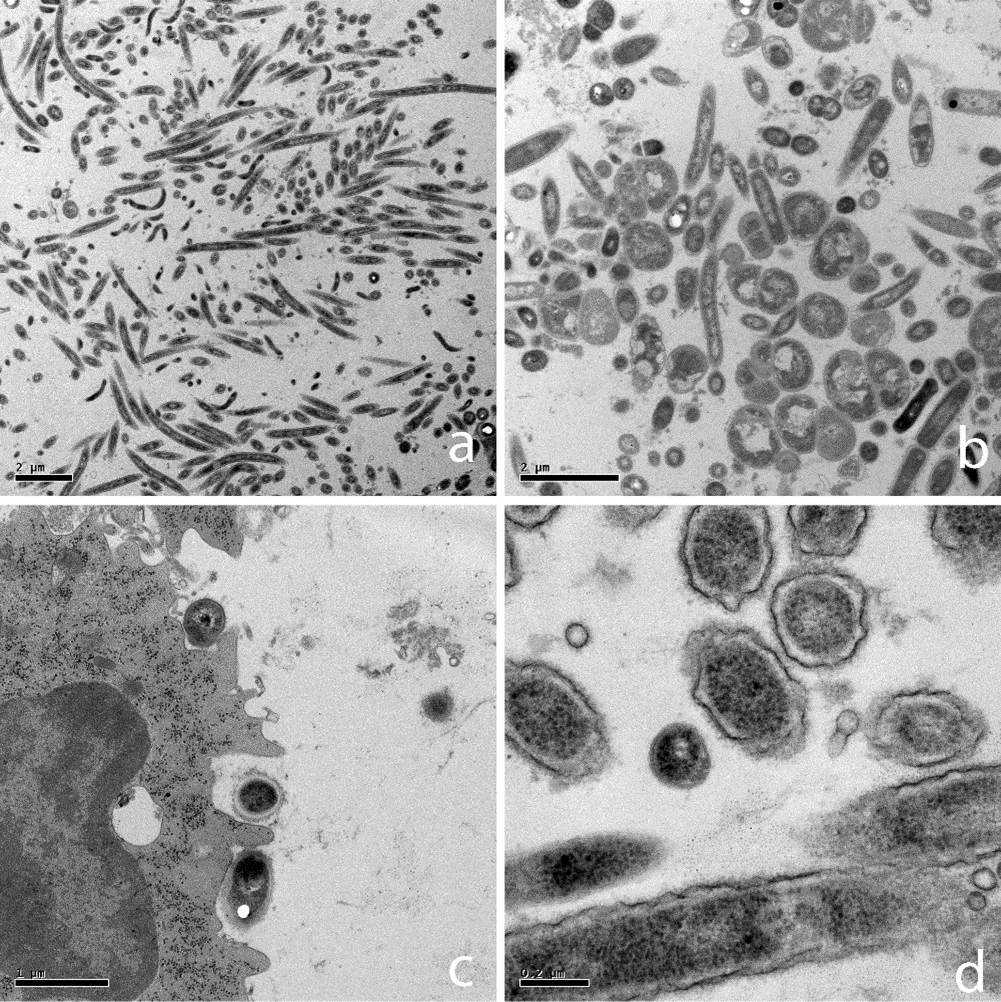
Figure 6: TEM Images of classical walled bacteria from chronic periodontitis individuals. a) Coccoid, fusiform, and few spirochete bacteria with classical cell wall morphology. 6000x. b) Coccoid and fusiform walled bacteria; 10000x. c) Leucocyte with various walled bacteria attached to his plasma membrane; 20000x. d) Gram-bacteria 80000x.
In samples processed for electron microscopy, CWDB were seen only in aggressive periodontitis individuals (Figures 2a-2h) while in chronic periodontitis individuals only walled bacteria were found (Figures 6a-6d). A variety of forms were found in each aggressive periodontitis sample. Range sizes vary from 0.2 μm to 10 μm. CWDB can be recognized by the presence of the plasma membrane bi-layer and the absence of the cell wall, as shown in (Figure 2e). In some cases, these organisms presented a light granular cytoplasm with small vesicles inside, possibly representing reproductive units (Figures 2a, 2b, 2g & 2h). The presence of small ribosome-like structure was also observed (Figures 6f-6h). CWDB were found inside granulocytes, and a representative image of many pleomorphic small forms inside a vacuole is shown in (Figures 2c & 2d). Larger CWDB presented small dark and light vesicles inside the cytoplasm and some could be seen outside the membrane layer (Figures 2g & 2h).
In samples processed for TEM with electron microscopy in situ hybridization, presence of bacterial DNA was seen in CWDB from aggressive periodontitis individuals (Figures 7a-7d). EDX microanalysis was also applied to confirm presence of gold particles (Data not shown). When we analysed biofilm culture samples, 2 from periodontally healthy individuals (G0), 2 from chronic periodontitis individuals (G0 and G1L) and 3 from aggressive periodontitis individuals (two G1L and one G1H), only in samples classified G1L and G1H we observed CWDB forms after filtration through 0,45 μm filters to exclude walled bacteria (Figure 8). In one filtered G1H sample we also detected motile CWDB (Movie S10).
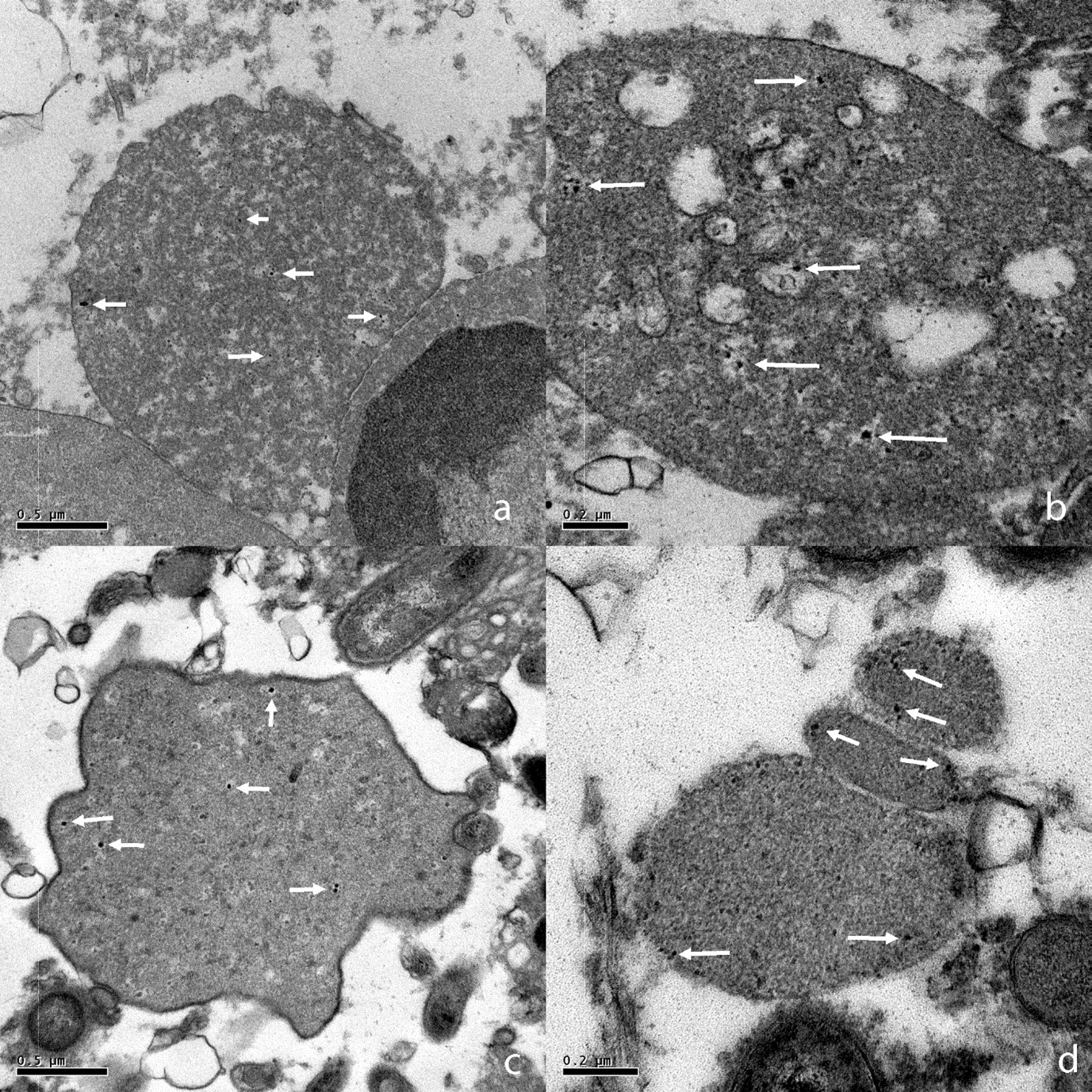
Figure 7: a-c) TEM in situ hybridization images (EUB 338 for 16S rRNA of most bacteria) of CWDB from aggressive periodontitis individuals (arrows indicate gold particles). a) CWDB with several gold particles inside cytoplasmic space adjacent to the membrane of leucocyte 50000X. b) CWDB with vacuoles inside cytoplasm 80000x. c) CWDB with a well conserved plasma membrane surrounded by walled bacteria 50000x. d) Three small CWDB 80000x.
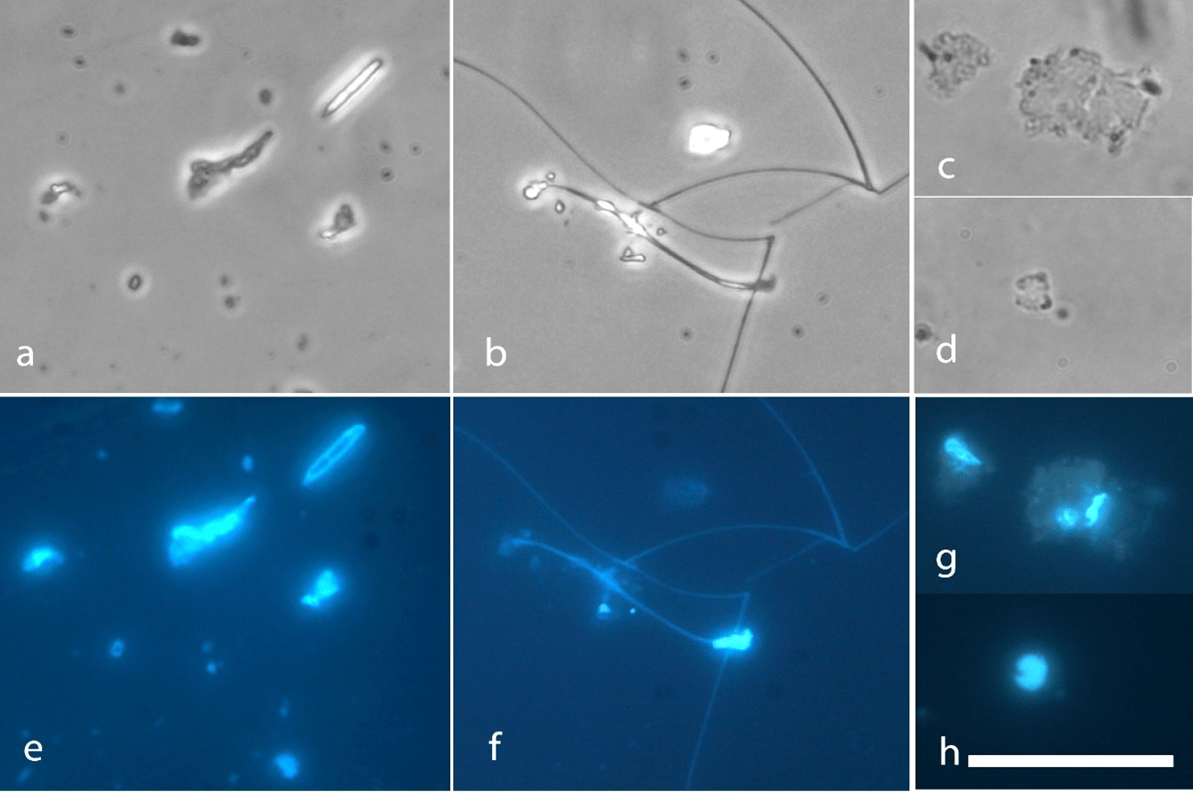
Figure 8: CWDB after culture and filtration with 0.45 μm filter. a) Protoplastic form. b) Filament form. c) & d) Damaged protoplastic form. e-h) Hoechst immunofluorescence staining of images above. Bar: 5 μm.
II Statistical Correlation Between CWDB and Individuals with Chronic or Aggressive Periodontal Disease and with Healthy Individuals
A sample of 89 individuals was evaluated (30 periodontally healthy, 36 with chronic periodontitis, and 23 with aggressive periodontitis). Figure 9 shows the number of patients presenting with CWDB. The results, listed below, were established after descriptive statistical evaluations were performed.
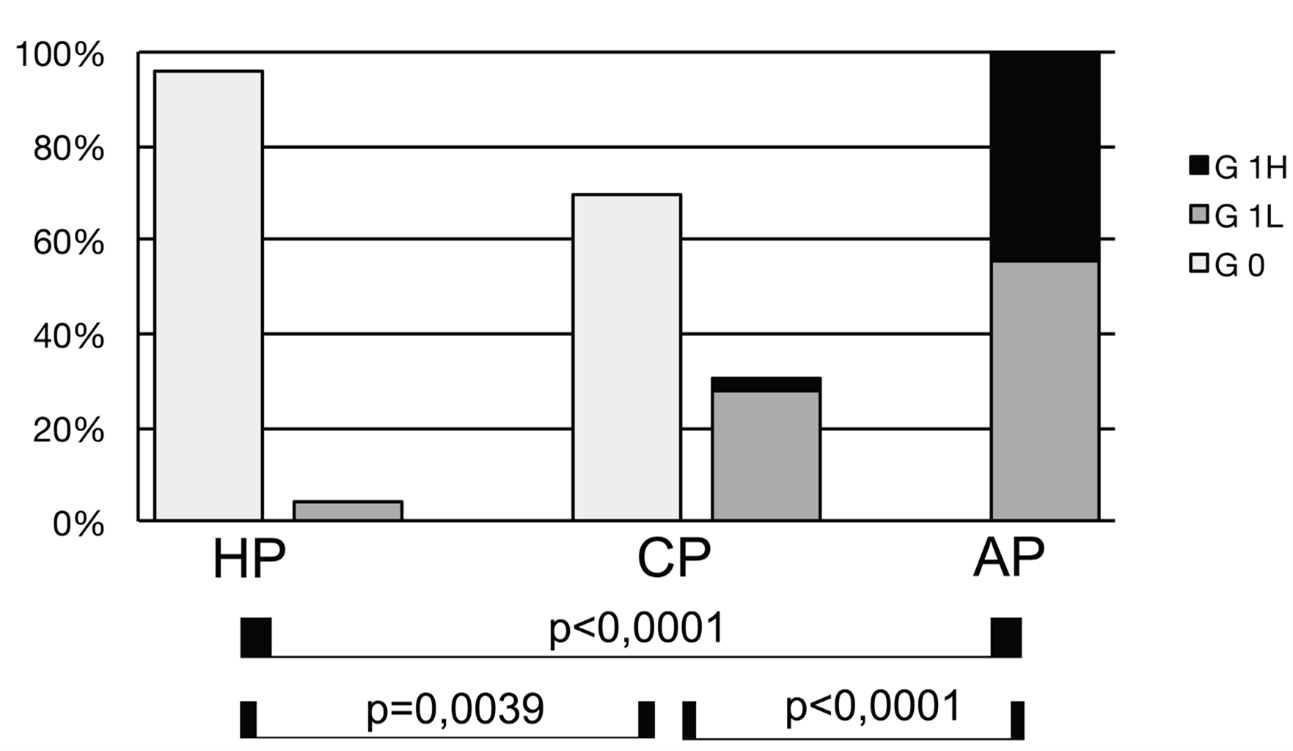
Figure 9: Association between CWDB and periodontal condition. G0: absence of CWDB or the presence of only protoplastic form without granules G1L: 2 kinds of CWDB were present or CWDB prevalence > 5%; G1H: 3 or more kinds of CWDB were present, or high prevalence of CWDB were found (> 70%). (see text for details). Periodontally Healthy (HP, n = 30), G0 = 29 (96.7%), G1L = 1 (3.3%), G1H = 0 (0%). Chronic periodontitis (CP, n = 36), G0 = 25 (69.4%), G1L = 10 (27.8%), G1H = 1 (2.8%). Aggressive periodontitis (AP, n = 23), G0 = 0 (0%), G1L = 12 (52.2%), G1H = 11 (47.8%).
The three groups showed the following values of CWDB: HP, G1 = 1 (3.3%); CP, G1 = 11 (30.6%); and AP, G1 = 23 (100%). The differences among the groups were statistically significant. Marked differences were found between HP and AP (chi-square = 49.10, p < .0001), between CP and AP (chi-square = 27.52, p < .0001), and between HP and CP (chi-square = 8.152, p = .00022). If we divide the G1 score in G1L and G1H, we have the highest G1H count in the AP group (G1L = 12, G1H = 11), while in CP only one sample presented this score (G1L = 10, G1H = 1).
To test the significance among the four kinds of CWDB we classified, we assessed the presence of each form in CP and AP groups positive for CWDB. We found no statistically significant correlation in the protoplastic, filament, and everted forms between the groups. Only intracellular forms showed a statistically significant correlation with the AP group (chi-square, 3.387; p = .032).
III PCR
To verify if CWDB are associated with known periodontal pathogenic bacteria, we assessed the prevalence of periodontopathic bacteria by means of polymerase chain-reaction (PCR). We found no clear, statistically significant, correlation among periodontal pathogens tested (except T. denticola, p = .005) that allowed individuals with chronic periodontitis to be distinguished from those with aggressive periodontitis (Figure 10).
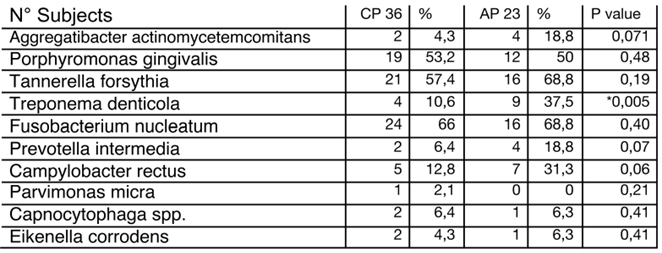
Figure 10: PCR of major periodontopathic bacteria analysed in chronic (CP) and aggressive (AP) periodontitis (P: significance of chi-square analysis; *statistically significant).
Discussion
Literature regarding CWDB in the oral cavity is not up to date and is based on unclear classifications, with terms such as PPLO, Mycoplasma, spheroplast, protoplast, and L-form often describing the same bacterial form. The majority of studies classifying and analysing CWDB used sophisticated culture techniques to select and maintain this bacterial state. To our knowledge, this is the first study linking CWDB to periodontal disease.
To overcome the difficulty and bias of the bacterial culture technique, we developed a simple method to verify morphology on fresh biofilm as well as the presence and prevalence of CWDB in periodontal disease according to the current classification, in which chronic and aggressive periodontitis are separate diseases. Since we know from the literature that a multitude of, if not all, bacteria can assume the CWD form, a molecular study to characterize those forms of bacteria in our sample was beyond the scope of this research.
The results demonstrated statistically significant results confirming a considerable association between CWDB and aggressive periodontitis, with a low association in periodontally healthy individuals and in those with chronic periodontitis. Another important observation was the presence of varieties related to the kind of periodontal disease: everted forms, filament forms, areas containing more than 80% of CWDB, erythrocyte associated forms and endonuclear invasion were consistently related to aggressive periodontitis (data not shown).
Our analyses of the relation between CWDB and healthy individuals and those with chronic and aggressive periodontitis showed that only aggressive periodontitis was highly associated with CWDB grade 1 values (100%, 23/23), while the associations in individuals with chronic periodontitis was low (30.6%, 11/36) and periodontally healthy individuals (4%, 1/30) was very low. These results could be connected to differences in terms of progression of periodontal destruction and severity of aggressive and chronic disease.
This was not surprising, because the transformation in CWDB can alter bacterial gene expression and can amplify virulence factors such as: horizontal gene transfer, capacity to penetrate host cells, stealthy entrance into the immune system. We now know that CWDB requires a combination of two kinds of mutations, one work by generating excess amounts of cell membrane and another work by stabilizing the proliferating CWDB and preventing them from lysing. Oxidative damage prevents growth of CWDB, and reduction of ROS levels or anaerobic conditions promotes their growth (Kawai et al. 2015). TEM images obtained from aggressive periodontitis samples showed that the variety of forms that CWDB take are similar to images seen, at lower magnification, with phase contrast microscope and to the ultrastructure of Mycoplasma and L-forms of bacteria [19-20].
Another interesting observation was the inhomogeneous distribution of DNA in the protoplastic forms, as tested with Hoechst staining, that was comparable with images obtained in Listeria monocytogenes cultures indicating intracellular vesicles as reproduction elements [30]. To test whether CWDB seen were true bacteria electron microscopy in situ hybridization with the EUB 338 probe, specific for general Eubacteria, on 9 samples (3 for each clinical groups analysed), only samples from aggressive periodontitis individuals shows CWDB. Which mechanisms induce the loss of cell walls in these bacteria? Some studies suggest that a component in the membrane of the L-form, distinct from cell wall components such as teichoic acid or lipopolysaccharide, possesses the capability to stimulate TNF-α production by macrophages [31-35]. The mechanisms of macrophage activation by the membranes of Mycoplasmas, were shown to increase TNF-α production [33].
Another study has demonstrated that a ‘hyperresponsive’ phenotype in individuals with localized aggressive periodontitis, upon activation by common periodontal pathogens, could contribute to exacerbated inflammatory responses and eventual rapid host tissue destruction [36]. Another study indicated differential immunoregulatory mechanisms in AP and CP, suggesting the presence of different cellular activation in the two different clinical forms [37]. These mechanisms could be related to distinct bacteria or antigens present during disease.
Our study results add another small piece to the multifactorial relationship between periodontal biofilm and host response, suggesting that CWDB are associated mainly with aggressive periodontitis. Further studies are needed for molecular characterization of these bacteria and clarification of whether CWDB are an effect of a specific host response or are capable of altered immune response. Ultimately, we believe that knowledge of the role of CWDB in periodontal disease could improve or help the diagnosis and development of new therapeutic protocols for these patients.
Acknowledgements
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sector.
Conflicts of Interest
None.
Table 1: Clinical Data for Individuals in the Study Population. (PD: Probing depth; CAL: Clinical attachment level; PI: Plaque index; BOP: Bleeding on probing; Kinds of CWDB forms; Gender; Age; CWDB grade). (CWDB: P: Protoplastic, E: Everted, F: Filament, I: Intracellular).
|
Periodontally Healthy |
Age |
Sex |
CWDB Grade |
P. |
E. |
F. |
I. |
PD |
CAL |
PI |
BOP |
Missing Teeth (n) |
|
HP1 |
55 |
f |
0 |
|
|
|
|
2,2 |
1,2 |
3,4 |
13,8 |
3 |
|
HP2 |
48 |
f |
0 |
|
|
|
|
1,4 |
1,2 |
3,6 |
14,3 |
4 |
|
HP3 |
36 |
f |
0 |
|
|
|
|
1,5 |
0,5 |
3,3 |
13,3 |
2 |
|
HP4 |
45 |
f |
0 |
|
|
|
|
2,6 |
1,5 |
13,8 |
17,2 |
3 |
|
HP5 |
25 |
f |
0 |
|
|
|
|
2,8 |
0,7 |
3,2 |
12,9 |
1 |
|
HP6 |
58 |
f |
0 |
|
|
|
|
2,6 |
1,3 |
6,9 |
13,8 |
3 |
|
HP7 |
46 |
m |
0 |
|
|
|
|
2,1 |
1,3 |
7,4 |
18,5 |
5 |
|
HP8 |
51 |
m |
0 |
|
|
|
|
2,8 |
1,4 |
6,9 |
13,8 |
3 |
|
HP9 |
66 |
m |
0 |
|
|
|
|
2,4 |
1,5 |
20,0 |
20,0 |
7 |
|
HP10 |
48 |
f |
0 |
|
|
|
|
2 |
1,2 |
7,1 |
17,9 |
4 |
|
HP11 |
55 |
f |
0 |
|
|
|
|
2 |
1,5 |
7,4 |
18,5 |
5 |
|
HP12 |
35 |
f |
0 |
|
|
|
|
2,4 |
0,4 |
6,7 |
13,3 |
2 |
|
HP13 |
66 |
m |
0 |
|
|
|
|
2,4 |
1,6 |
6,9 |
17,2 |
3 |
|
HP14 |
64 |
m |
0 |
|
|
|
|
2,5 |
1,3 |
7,1 |
17,9 |
4 |
|
HP15 |
42 |
f |
0 |
|
|
|
|
1,6 |
0,4 |
6,9 |
17,2 |
3 |
|
HP16 |
45 |
f |
0 |
|
|
|
|
2 |
0,5 |
6,9 |
13,8 |
3 |
|
HP17 |
41 |
f |
0 |
|
|
|
|
2,7 |
0,7 |
14,8 |
22,2 |
5 |
|
HP18 |
38 |
f |
0 |
|
|
|
|
2,4 |
1,3 |
3,4 |
13,8 |
3 |
|
HP19 |
39 |
f |
0 |
|
|
|
|
2 |
1,5 |
3,6 |
14,3 |
4 |
|
HP20 |
55 |
m |
0 |
|
|
|
|
2,1 |
0,8 |
3,8 |
15,4 |
6 |
|
HP21 |
67 |
f |
0 |
|
|
|
|
2,6 |
1,8 |
7,7 |
15,4 |
6 |
|
HP22 |
35 |
m |
1L |
* |
|
|
* |
2,5 |
0,8 |
6,9 |
13,8 |
3 |
|
HP23 |
55 |
m |
0 |
|
|
|
|
2,4 |
1,5 |
13,8 |
24,1 |
3 |
|
HP24 |
68 |
m |
0 |
|
|
|
|
2,2 |
0,4 |
14,8 |
18,5 |
5 |
|
HP25 |
55 |
m |
0 |
|
|
|
|
2,6 |
1,5 |
7,1 |
14,3 |
4 |
|
HP26 |
51 |
m |
0 |
|
|
|
|
2,2 |
0,9 |
10,7 |
14,3 |
4 |
|
HP27 |
55 |
m |
0 |
|
|
|
|
1,9 |
0,5 |
3,4 |
6,9 |
3 |
|
HP28 |
64 |
m |
0 |
|
|
|
|
2,3 |
1,9 |
7,1 |
14,3 |
4 |
|
HP29 |
57 |
m |
0 |
|
|
|
|
2,3 |
0,9 |
10,7 |
17,9 |
4 |
|
HP30 |
65 |
m |
0 |
|
|
|
|
2,1 |
2 |
18,5 |
14,8 |
5 |
|
N° Samples |
Mean Age |
W/M |
|
Tot. |
Tot. |
Tot. |
Tot. |
PD±SD |
CAL ±SD |
PI (%± SD) |
BOP (%±SD) |
MT± SD |
|
30 |
51 |
15/15 |
|
1 |
0 |
0 |
1 |
2,25±0,4 |
1,1±0,5 |
8,4±4,6 |
15,7±3,2 |
3,8±1,3 |
|
Chronic Periodontitis |
Age |
Sex |
CWDB Grade |
P. |
E. |
F. |
I. |
PD |
CAL |
PI |
BOP |
Missing Teeth (n) |
|
CP1 |
36 |
f |
1L |
* |
|
|
* |
2,3 |
2,9 |
33,3 |
63,0 |
5 |
|
CP2 |
55 |
m |
0 |
|
|
|
|
3,9 |
3,6 |
45,8 |
50,0 |
8 |
|
CP3 |
58 |
m |
0 |
|
|
|
|
2,8 |
3,3 |
45,8 |
54,2 |
8 |
|
CP4 |
70 |
m |
1L |
* |
* |
|
* |
3,3 |
3,6 |
52,2 |
39,1 |
9 |
|
CP5 |
72 |
f |
1L |
* |
|
|
* |
2 |
3,2 |
54,5 |
52,4 |
11 |
|
CP6 |
75 |
f |
1L |
* |
|
|
|
3 |
3,4 |
45,5 |
50,0 |
10 |
|
CP7 |
56 |
m |
0 |
|
|
|
|
3,6 |
3,9 |
52,2 |
56,5 |
9 |
|
CP8 |
48 |
f |
1H |
* |
|
* |
|
2,3 |
2,6 |
56,5 |
56,5 |
9 |
|
CP9 |
67 |
m |
1L |
* |
|
* |
|
5,1 |
5,6 |
52,2 |
65,2 |
9 |
|
C10 |
44 |
m |
0 |
|
|
|
|
3,2 |
3,7 |
41,7 |
54,2 |
8 |
|
CP11 |
55 |
f |
1L |
* |
|
|
* |
2,9 |
3,4 |
50,0 |
54,5 |
10 |
|
CP12 |
50 |
m |
0 |
|
|
|
|
3,9 |
4,6 |
50,0 |
54,5 |
10 |
|
CP13 |
43 |
f |
0 |
|
|
|
|
5 |
5,3 |
69,6 |
60,9 |
9 |
|
CP14 |
48 |
f |
0 |
|
|
|
|
4,1 |
4,6 |
69,6 |
56,5 |
9 |
|
CP15 |
55 |
m |
1L |
* |
|
|
|
4 |
4,7 |
60,0 |
60,0 |
12 |
|
CP16 |
67 |
f |
0 |
|
|
|
|
5 |
4,8 |
52,2 |
47,8 |
9 |
|
CP17 |
58 |
f |
1L |
* |
|
|
|
4,1 |
5,1 |
56,5 |
52,2 |
9 |
|
CP18 |
69 |
m |
0 |
|
|
|
|
3,8 |
4,8 |
34,6 |
42,3 |
6 |
|
CP19 |
59 |
m |
0 |
|
|
|
|
4,3 |
5,5 |
43,5 |
52,2 |
9 |
|
CP20 |
49 |
f |
0 |
|
|
|
|
4 |
4,4 |
52,4 |
52,4 |
11 |
|
CP21 |
43 |
f |
0 |
|
|
|
|
4 |
4,5 |
38,1 |
47,6 |
11 |
|
CP22 |
56 |
m |
0 |
|
|
|
|
4,7 |
5,3 |
39,1 |
52,2 |
9 |
|
CP23 |
70 |
m |
0 |
|
|
|
|
4,4 |
5 |
47,8 |
43,5 |
9 |
|
CP24 |
71 |
m |
0 |
|
|
|
|
4,2 |
5,3 |
40,0 |
44,0 |
7 |
|
CP25 |
53 |
m |
0 |
|
|
|
|
4,1 |
5,5 |
43,5 |
47,8 |
9 |
|
CP26 |
66 |
f |
0 |
|
|
|
|
4,1 |
4,8 |
54,5 |
45,5 |
10 |
|
CP27 |
52 |
m |
1L |
* |
|
|
|
3,6 |
4,7 |
50,0 |
50,0 |
8 |
|
CP28 |
60 |
f |
0 |
|
|
|
|
5,7 |
6,3 |
52,2 |
52,2 |
9 |
|
CP29 |
59 |
m |
0 |
|
|
|
|
4,5 |
5,1 |
40,7 |
48,1 |
5 |
|
CP30 |
64 |
f |
1L |
* |
|
|
|
4,4 |
4,9 |
47,8 |
47,8 |
9 |
|
CP31 |
61 |
m |
0 |
|
|
|
|
3 |
3,3 |
40,9 |
45,5 |
10 |
|
CP32 |
54 |
m |
0 |
|
|
|
|
2,5 |
3 |
39,1 |
52,2 |
9 |
|
CP33 |
50 |
m |
0 |
|
|
|
|
4,7 |
5,4 |
33,3 |
50,0 |
8 |
|
CP34 |
49 |
m |
0 |
|
|
|
* |
4,9 |
5,4 |
43,5 |
65,2 |
9 |
|
CP35 |
58 |
m |
0 |
|
|
|
|
5 |
6,6 |
52,4 |
52,4 |
11 |
|
CP36 |
60 |
m |
0 |
|
|
|
|
4,1 |
4,8 |
47,6 |
47,6 |
11 |
|
N° samples |
Mean Age |
W/M |
|
Tot. |
Tot. |
Tot. |
Tot. |
PD±SD |
CAL ±SD |
PI (%± SD) |
BOP (%±SD) |
MT± SD |
|
36 |
57,2 |
14/22 |
|
11 |
1 |
2 |
5 |
3,9 ±0,9 |
4,5 ±1 |
48 ±8,6 |
51,8 ±6,1 |
9 ±1,5 |
|
Aggressive Periodontitis |
Age |
Sex |
CWDB Grade |
P. |
E. |
F. |
I. |
PD |
CAL |
PI |
BOP |
Missing Teeth (n) |
|
AgP1 |
35 |
f |
1H |
* |
* |
* |
|
4 |
4,2 |
41,7 |
70,8 |
8 |
|
AgP2 |
32 |
f |
1H |
* |
|
* |
|
4,5 |
2,9 |
42,3 |
53,8 |
6 |
|
AgP3 |
31 |
f |
1L |
* |
|
|
* |
2,7 |
2,3 |
33,3 |
55,6 |
5 |
|
AgP4 |
34 |
f |
1H |
* |
|
|
* |
5,1 |
5,4 |
50,0 |
53,8 |
6 |
|
AgP5 |
25 |
f |
1L |
* |
|
|
* |
4 |
3 |
40,7 |
74,1 |
5 |
|
AgP6 |
31 |
f |
1L |
* |
|
|
* |
3,6 |
3,4 |
57,7 |
61,5 |
6 |
|
AgP7 |
34 |
m |
1L |
* |
|
|
* |
3,6 |
5 |
40,0 |
48,0 |
7 |
|
AgP8 |
33 |
m |
1L |
* |
|
|
* |
2,6 |
3,9 |
44,0 |
72,0 |
7 |
|
AgP9 |
30 |
m |
1H |
* |
* |
|
|
5,2 |
5,3 |
37,5 |
62,5 |
8 |
|
AgP10 |
34 |
f |
1H |
* |
* |
|
* |
3,8 |
5,5 |
66,7 |
66,7 |
5 |
|
AgP11 |
35 |
f |
1H |
* |
|
|
* |
4,6 |
5 |
45,8 |
45,8 |
8 |
|
AgP12 |
29 |
f |
1L |
* |
|
|
|
3,1 |
3,3 |
29,6 |
70,4 |
5 |
|
AgP13 |
34 |
m |
1L |
* |
* |
|
|
3 |
4,3 |
46,2 |
46,2 |
6 |
|
AgP14 |
35 |
m |
1H |
* |
* |
|
|
2,8 |
3,1 |
35,7 |
50,0 |
4 |
|
AgP15 |
32 |
f |
1H |
* |
* |
|
* |
4,6 |
5 |
60,0 |
60,0 |
7 |
|
AgP16 |
29 |
f |
1L |
* |
|
|
|
3,4 |
4,3 |
41,7 |
54,2 |
8 |
|
AgP17 |
34 |
f |
1H |
* |
|
|
* |
4,2 |
4,3 |
41,7 |
50,0 |
8 |
|
AgP18 |
34 |
f |
1L |
* |
|
|
* |
4 |
4,3 |
73,1 |
65,4 |
6 |
|
AgP19 |
35 |
f |
1H |
* |
|
|
* |
4,5 |
4,8 |
40,0 |
52,0 |
7 |
|
AgP20 |
27 |
m |
1L |
* |
|
|
* |
3,6 |
5,2 |
52,2 |
87,0 |
9 |
|
AgP21 |
31 |
f |
1L |
* |
|
|
* |
3,7 |
4,2 |
34,6 |
50,0 |
6 |
|
AgP22 |
24 |
f |
1H |
* |
|
* |
* |
2,6 |
1,6 |
24,1 |
72,4 |
3 |
|
AgP23 |
34 |
f |
1L |
* |
|
|
* |
4 |
5 |
40,7 |
48,1 |
5 |
|
N° samples |
Mean Age |
W/M |
|
Tot. |
Tot. |
Tot. |
Tot. |
PD±SD |
CAL ±SD |
PI (%± SD) |
BOP (%±SD) |
MT± SD |
|
23 |
31,8 |
17/6 |
|
23 |
6 |
3 |
16 |
3,8 ±0,8 |
4,1 ±1,1 |
44,3 ±11,5 |
59,6 ±11,1 |
6,3 ±1,5 |
Article Info
Article Type
Research ArticlePublication history
Received: Mon 23, Nov 2020Accepted: Fri 04, Dec 2020
Published: Tue 15, Dec 2020
Copyright
© 2023 Francesco Germano. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.DOBCR.2020.06.03
Figures & Tables
Table 1: Clinical Data for Individuals in the Study Population. (PD: Probing depth; CAL: Clinical attachment level; PI: Plaque index; BOP: Bleeding on probing; Kinds of CWDB forms; Gender; Age; CWDB grade). (CWDB: P: Protoplastic, E: Everted, F: Filament, I: Intracellular).
|
Periodontally Healthy |
Age |
Sex |
CWDB Grade |
P. |
E. |
F. |
I. |
PD |
CAL |
PI |
BOP |
Missing Teeth (n) |
|
HP1 |
55 |
f |
0 |
|
|
|
|
2,2 |
1,2 |
3,4 |
13,8 |
3 |
|
HP2 |
48 |
f |
0 |
|
|
|
|
1,4 |
1,2 |
3,6 |
14,3 |
4 |
|
HP3 |
36 |
f |
0 |
|
|
|
|
1,5 |
0,5 |
3,3 |
13,3 |
2 |
|
HP4 |
45 |
f |
0 |
|
|
|
|
2,6 |
1,5 |
13,8 |
17,2 |
3 |
|
HP5 |
25 |
f |
0 |
|
|
|
|
2,8 |
0,7 |
3,2 |
12,9 |
1 |
|
HP6 |
58 |
f |
0 |
|
|
|
|
2,6 |
1,3 |
6,9 |
13,8 |
3 |
|
HP7 |
46 |
m |
0 |
|
|
|
|
2,1 |
1,3 |
7,4 |
18,5 |
5 |
|
HP8 |
51 |
m |
0 |
|
|
|
|
2,8 |
1,4 |
6,9 |
13,8 |
3 |
|
HP9 |
66 |
m |
0 |
|
|
|
|
2,4 |
1,5 |
20,0 |
20,0 |
7 |
|
HP10 |
48 |
f |
0 |
|
|
|
|
2 |
1,2 |
7,1 |
17,9 |
4 |
|
HP11 |
55 |
f |
0 |
|
|
|
|
2 |
1,5 |
7,4 |
18,5 |
5 |
|
HP12 |
35 |
f |
0 |
|
|
|
|
2,4 |
0,4 |
6,7 |
13,3 |
2 |
|
HP13 |
66 |
m |
0 |
|
|
|
|
2,4 |
1,6 |
6,9 |
17,2 |
3 |
|
HP14 |
64 |
m |
0 |
|
|
|
|
2,5 |
1,3 |
7,1 |
17,9 |
4 |
|
HP15 |
42 |
f |
0 |
|
|
|
|
1,6 |
0,4 |
6,9 |
17,2 |
3 |
|
HP16 |
45 |
f |
0 |
|
|
|
|
2 |
0,5 |
6,9 |
13,8 |
3 |
|
HP17 |
41 |
f |
0 |
|
|
|
|
2,7 |
0,7 |
14,8 |
22,2 |
5 |
|
HP18 |
38 |
f |
0 |
|
|
|
|
2,4 |
1,3 |
3,4 |
13,8 |
3 |
|
HP19 |
39 |
f |
0 |
|
|
|
|
2 |
1,5 |
3,6 |
14,3 |
4 |
|
HP20 |
55 |
m |
0 |
|
|
|
|
2,1 |
0,8 |
3,8 |
15,4 |
6 |
|
HP21 |
67 |
f |
0 |
|
|
|
|
2,6 |
1,8 |
7,7 |
15,4 |
6 |
|
HP22 |
35 |
m |
1L |
* |
|
|
* |
2,5 |
0,8 |
6,9 |
13,8 |
3 |
|
HP23 |
55 |
m |
0 |
|
|
|
|
2,4 |
1,5 |
13,8 |
24,1 |
3 |
|
HP24 |
68 |
m |
0 |
|
|
|
|
2,2 |
0,4 |
14,8 |
18,5 |
5 |
|
HP25 |
55 |
m |
0 |
|
|
|
|
2,6 |
1,5 |
7,1 |
14,3 |
4 |
|
HP26 |
51 |
m |
0 |
|
|
|
|
2,2 |
0,9 |
10,7 |
14,3 |
4 |
|
HP27 |
55 |
m |
0 |
|
|
|
|
1,9 |
0,5 |
3,4 |
6,9 |
3 |
|
HP28 |
64 |
m |
0 |
|
|
|
|
2,3 |
1,9 |
7,1 |
14,3 |
4 |
|
HP29 |
57 |
m |
0 |
|
|
|
|
2,3 |
0,9 |
10,7 |
17,9 |
4 |
|
HP30 |
65 |
m |
0 |
|
|
|
|
2,1 |
2 |
18,5 |
14,8 |
5 |
|
N° Samples |
Mean Age |
W/M |
|
Tot. |
Tot. |
Tot. |
Tot. |
PD±SD |
CAL ±SD |
PI (%± SD) |
BOP (%±SD) |
MT± SD |
|
30 |
51 |
15/15 |
|
1 |
0 |
0 |
1 |
2,25±0,4 |
1,1±0,5 |
8,4±4,6 |
15,7±3,2 |
3,8±1,3 |
|
Chronic Periodontitis |
Age |
Sex |
CWDB Grade |
P. |
E. |
F. |
I. |
PD |
CAL |
PI |
BOP |
Missing Teeth (n) |
|
CP1 |
36 |
f |
1L |
* |
|
|
* |
2,3 |
2,9 |
33,3 |
63,0 |
5 |
|
CP2 |
55 |
m |
0 |
|
|
|
|
3,9 |
3,6 |
45,8 |
50,0 |
8 |
|
CP3 |
58 |
m |
0 |
|
|
|
|
2,8 |
3,3 |
45,8 |
54,2 |
8 |
|
CP4 |
70 |
m |
1L |
* |
* |
|
* |
3,3 |
3,6 |
52,2 |
39,1 |
9 |
|
CP5 |
72 |
f |
1L |
* |
|
|
* |
2 |
3,2 |
54,5 |
52,4 |
11 |
|
CP6 |
75 |
f |
1L |
* |
|
|
|
3 |
3,4 |
45,5 |
50,0 |
10 |
|
CP7 |
56 |
m |
0 |
|
|
|
|
3,6 |
3,9 |
52,2 |
56,5 |
9 |
|
CP8 |
48 |
f |
1H |
* |
|
* |
|
2,3 |
2,6 |
56,5 |
56,5 |
9 |
|
CP9 |
67 |
m |
1L |
* |
|
* |
|
5,1 |
5,6 |
52,2 |
65,2 |
9 |
|
C10 |
44 |
m |
0 |
|
|
|
|
3,2 |
3,7 |
41,7 |
54,2 |
8 |
|
CP11 |
55 |
f |
1L |
* |
|
|
* |
2,9 |
3,4 |
50,0 |
54,5 |
10 |
|
CP12 |
50 |
m |
0 |
|
|
|
|
3,9 |
4,6 |
50,0 |
54,5 |
10 |
|
CP13 |
43 |
f |
0 |
|
|
|
|
5 |
5,3 |
69,6 |
60,9 |
9 |
|
CP14 |
48 |
f |
0 |
|
|
|
|
4,1 |
4,6 |
69,6 |
56,5 |
9 |
|
CP15 |
55 |
m |
1L |
* |
|
|
|
4 |
4,7 |
60,0 |
60,0 |
12 |
|
CP16 |
67 |
f |
0 |
|
|
|
|
5 |
4,8 |
52,2 |
47,8 |
9 |
|
CP17 |
58 |
f |
1L |
* |
|
|
|
4,1 |
5,1 |
56,5 |
52,2 |
9 |
|
CP18 |
69 |
m |
0 |
|
|
|
|
3,8 |
4,8 |
34,6 |
42,3 |
6 |
|
CP19 |
59 |
m |
0 |
|
|
|
|
4,3 |
5,5 |
43,5 |
52,2 |
9 |
|
CP20 |
49 |
f |
0 |
|
|
|
|
4 |
4,4 |
52,4 |
52,4 |
11 |
|
CP21 |
43 |
f |
0 |
|
|
|
|
4 |
4,5 |
38,1 |
47,6 |
11 |
|
CP22 |
56 |
m |
0 |
|
|
|
|
4,7 |
5,3 |
39,1 |
52,2 |
9 |
|
CP23 |
70 |
m |
0 |
|
|
|
|
4,4 |
5 |
47,8 |
43,5 |
9 |
|
CP24 |
71 |
m |
0 |
|
|
|
|
4,2 |
5,3 |
40,0 |
44,0 |
7 |
|
CP25 |
53 |
m |
0 |
|
|
|
|
4,1 |
5,5 |
43,5 |
47,8 |
9 |
|
CP26 |
66 |
f |
0 |
|
|
|
|
4,1 |
4,8 |
54,5 |
45,5 |
10 |
|
CP27 |
52 |
m |
1L |
* |
|
|
|
3,6 |
4,7 |
50,0 |
50,0 |
8 |
|
CP28 |
60 |
f |
0 |
|
|
|
|
5,7 |
6,3 |
52,2 |
52,2 |
9 |
|
CP29 |
59 |
m |
0 |
|
|
|
|
4,5 |
5,1 |
40,7 |
48,1 |
5 |
|
CP30 |
64 |
f |
1L |
* |
|
|
|
4,4 |
4,9 |
47,8 |
47,8 |
9 |
|
CP31 |
61 |
m |
0 |
|
|
|
|
3 |
3,3 |
40,9 |
45,5 |
10 |
|
CP32 |
54 |
m |
0 |
|
|
|
|
2,5 |
3 |
39,1 |
52,2 |
9 |
|
CP33 |
50 |
m |
0 |
|
|
|
|
4,7 |
5,4 |
33,3 |
50,0 |
8 |
|
CP34 |
49 |
m |
0 |
|
|
|
* |
4,9 |
5,4 |
43,5 |
65,2 |
9 |
|
CP35 |
58 |
m |
0 |
|
|
|
|
5 |
6,6 |
52,4 |
52,4 |
11 |
|
CP36 |
60 |
m |
0 |
|
|
|
|
4,1 |
4,8 |
47,6 |
47,6 |
11 |
|
N° samples |
Mean Age |
W/M |
|
Tot. |
Tot. |
Tot. |
Tot. |
PD±SD |
CAL ±SD |
PI (%± SD) |
BOP (%±SD) |
MT± SD |
|
36 |
57,2 |
14/22 |
|
11 |
1 |
2 |
5 |
3,9 ±0,9 |
4,5 ±1 |
48 ±8,6 |
51,8 ±6,1 |
9 ±1,5 |
|
Aggressive Periodontitis |
Age |
Sex |
CWDB Grade |
P. |
E. |
F. |
I. |
PD |
CAL |
PI |
BOP |
Missing Teeth (n) |
|
AgP1 |
35 |
f |
1H |
* |
* |
* |
|
4 |
4,2 |
41,7 |
70,8 |
8 |
|
AgP2 |
32 |
f |
1H |
* |
|
* |
|
4,5 |
2,9 |
42,3 |
53,8 |
6 |
|
AgP3 |
31 |
f |
1L |
* |
|
|
* |
2,7 |
2,3 |
33,3 |
55,6 |
5 |
|
AgP4 |
34 |
f |
1H |
* |
|
|
* |
5,1 |
5,4 |
50,0 |
53,8 |
6 |
|
AgP5 |
25 |
f |
1L |
* |
|
|
* |
4 |
3 |
40,7 |
74,1 |
5 |
|
AgP6 |
31 |
f |
1L |
* |
|
|
* |
3,6 |
3,4 |
57,7 |
61,5 |
6 |
|
AgP7 |
34 |
m |
1L |
* |
|
|
* |
3,6 |
5 |
40,0 |
48,0 |
7 |
|
AgP8 |
33 |
m |
1L |
* |
|
|
* |
2,6 |
3,9 |
44,0 |
72,0 |
7 |
|
AgP9 |
30 |
m |
1H |
* |
* |
|
|
5,2 |
5,3 |
37,5 |
62,5 |
8 |
|
AgP10 |
34 |
f |
1H |
* |
* |
|
* |
3,8 |
5,5 |
66,7 |
66,7 |
5 |
|
AgP11 |
35 |
f |
1H |
* |
|
|
* |
4,6 |
5 |
45,8 |
45,8 |
8 |
|
AgP12 |
29 |
f |
1L |
* |
|
|
|
3,1 |
3,3 |
29,6 |
70,4 |
5 |
|
AgP13 |
34 |
m |
1L |
* |
* |
|
|
3 |
4,3 |
46,2 |
46,2 |
6 |
|
AgP14 |
35 |
m |
1H |
* |
* |
|
|
2,8 |
3,1 |
35,7 |
50,0 |
4 |
|
AgP15 |
32 |
f |
1H |
* |
* |
|
* |
4,6 |
5 |
60,0 |
60,0 |
7 |
|
AgP16 |
29 |
f |
1L |
* |
|
|
|
3,4 |
4,3 |
41,7 |
54,2 |
8 |
|
AgP17 |
34 |
f |
1H |
* |
|
|
* |
4,2 |
4,3 |
41,7 |
50,0 |
8 |
|
AgP18 |
34 |
f |
1L |
* |
|
|
* |
4 |
4,3 |
73,1 |
65,4 |
6 |
|
AgP19 |
35 |
f |
1H |
* |
|
|
* |
4,5 |
4,8 |
40,0 |
52,0 |
7 |
|
AgP20 |
27 |
m |
1L |
* |
|
|
* |
3,6 |
5,2 |
52,2 |
87,0 |
9 |
|
AgP21 |
31 |
f |
1L |
* |
|
|
* |
3,7 |
4,2 |
34,6 |
50,0 |
6 |
|
AgP22 |
24 |
f |
1H |
* |
|
* |
* |
2,6 |
1,6 |
24,1 |
72,4 |
3 |
|
AgP23 |
34 |
f |
1L |
* |
|
|
* |
4 |
5 |
40,7 |
48,1 |
5 |
|
N° samples |
Mean Age |
W/M |
|
Tot. |
Tot. |
Tot. |
Tot. |
PD±SD |
CAL ±SD |
PI (%± SD) |
BOP (%±SD) |
MT± SD |
|
23 |
31,8 |
17/6 |
|
23 |
6 |
3 |
16 |
3,8 ±0,8 |
4,1 ±1,1 |
44,3 ±11,5 |
59,6 ±11,1 |
6,3 ±1,5 |
References
- Open Biol 3: 120143. [Crossref]
- Chen T, Yu WH, Izard J, Baranova OV, Lakshmanan A et al. (2010) The Human Oral Microbiome Database: a web accessible resource for investigating oral microbe taxonomic and genomic information. Database 2010: baq013. [Crossref]
- Sr GJD, Woody HB (1997) Bacterial persistence and expression of disease. Clin Microbiol Rev 10: 320-344. [Crossref]
- Onwuamaegbu ME, Belcher RA, Soare C (2005) Cell wall-deficient bacteria as a cause of infections: a review of the clinical significance. J Int Med Res 33: 1-20. [Crossref]
- Razin S, Yogev D, Naot Y (1998) Molecular biology and pathogenicity of mycoplasmas. Microbiol Mol Biol Rev 62: 1094-1156. [Crossref]
- Razin S, Michmann J, Shimshoni Z (1964) The occurrence of mycoplasma (pleuropneumonia-like organisms, PPLO) in the oral cavity of dentulous and edentulous subjects. J Dent Res 43: 402-405. [Crossref]
- Watanabe T, Matsuura M, Seto K (1986) Enumeration, isolation, and species identification of mycoplasmas in saliva sampled from the normal and pathological human oral cavity and antibody response to an oral mycoplasma (Mycoplasma salivarium). J Clin Microbiol 23: 1034-1038. [Crossref]
- Kwek HS, Wilson M, Newman HN (1990) Mycoplasma in relation to gingivitis and periodontitis. J Clin Periodontol 17: 119-122. [Crossref]
- Newman MG, Saglie R, Jr FAC, Kaufman AK (1984) Mycoplasma in periodontal disease: isolation in juvenile Periodontitis. J Periodontol 55: 574-580. [Crossref]
- Kleinberger E (1935) The natural occurrence of pleuropneumonia-like organisms in apparent symbiosis with Streptobacillus moniliformis and other bacteria. J Pathol Bacteriol 40: 93-105.
- Allan EJ, Hoischen C, Gumpert J (2009) Bacterial L-forms. Adv Appl Microbiol 68: 1-39. [Crossref]
- Mercier R, Kawai Y, Errington J (2013) Excess membrane synthesis drives a primitive mode of cell proliferation. Cell 152: 997-1007. [Crossref]
- Cambre A, Zimmermann M, Sauer U, Vivijs B, Cenens Wet al. (2015) Metabolite profiling and peptidoglycan analysis of transient cell wall-deficient bacteria in a new Escherichia coli model system. Environ Microbiol. [Crossref]
- Markova N, Slavchev G, Michailova L, Jourdanova M (2010) Survival of Escherichia coli under lethal heat stress by L-form conversion. Int J Biolog Sci 6: 303-315. [Crossref]
- Kagan CY, Mikhailova VS (1963) Isolation of L-forms of streptococci from blood of patients with rheumatism and endocarditis. J Hyg Epidemiol Microbiol Immunol 7: 327-343. [Crossref]
- Gordon SL, Greer RB, Craig CP (1971) Recurrent osteomyelitis: report of four cases culturing L form variants of staphylococci. J Bone Joint Surg Am 53: 1150-1156. [Crossref]
- MacDonald AB (1988) Concurrent neocortical borreliosis and Alzheimer's disease: demonstration of a spirochetal cyst form. Ann NY Acad Sci 539: 468-470.
- Macomber PB (1990) Cancer and cell wall deficient bacteria. Med Hypotheses 32: 1-9. [Crossref]
- Anderson DR, Barile MF (1965) Ultrastructure of Mycoplasma hominis. J Bacteriol 90: 180-192. [Crossref]
- Dienes L, Bullivant S (1968) Morphology and reproductive processes of the L forms of bacteria. II. Comparative study of L forms and Mycoplasma with the electron microscope. J Bacteriol 95: 672-687. [Crossref]
- Mombelli A, Casagni F, Madianos PN (2002) Can presence or absence of periodontal pathogens distinguish between subjects with chronic and aggressive periodontitis? A systematic review. J Clin Periodontol 3: 10-21. [Crossref]
- Armitage GC (1999) Development of a classification system for periodontal diseases and conditions. Ann Periodontol 4: 1-6. [Crossref]
- Germano F, Bramanti E, Arcuri C, Cecchetti F, Cicciù M (2013) Atomic force microscopy of bacteria from periodontal subgingival biofilm: preliminary study results. Eur J Dent 7: 152-158. [Crossref]
- Armitage GC, Cullinan MP (2010) Comparison of the clinical features of chronic and aggressive periodontitis. Periodontol 2000 53: 12-27. [Crossref]
- Demmer RT, Papapanou PN (2010) Epidemiologic patterns of chronic and aggressive periodontitis. Periodontol 2000 53: 28-44. [Crossref].
- Eick S, Pfister W (2002) Comparison of microbial cultivation and a commercial PCR based method for detection of periodontopathogenic species in subgingival plaque samples. J Clin Periodontol 29: 638-644. [Crossref]
- Scimeca M, Giannini E, Antonacci C, Pistolese CA, Spagnoli LG et al. (2014) Microcalcifications in breast cancer: an active phenomenon mediated by epithelial cells with mesenchymal characteristics. BMC Cancer 14: 286. [Crossref]
- Reynolds ES (1963) The use of lead citrate at high pH as an electron-opaque stain in electron microscopy. J Cell Biol 17: 208-212. [Crossref]
- Mattman LH (2001) Stealth pathogens. 3rd ed. Boca Raton, FL: CRC Press.
- Briers Y, Staubli T, Schmid MC, Wagner M, Schuppler M et al. (2012) Intracellular Vesicles as Reproduction Elements in Cell Wall-Deficient L-Form Bacteria. PLoS One 7: e38514. [Crossref]
- Gallily R, Sher T, Av PB, Loewenstein J (1989) Tumor necrosis factor as a mediator of Mycoplasma orale-induced tumor cell lysis by macrophages. Cell Immunol 121: 146-153. [Crossref]
- Arai S, Furukawa M, Munakata T, Kuwano K, Inoue H et al. (1990) Enhancement of cytotoxicity of active macrophages by mycoplasma: role of mycoplasma-associated induction of tumor necrosis factor-α (TNF-α) in macrophages. Microbiol Immunol 34: 231-243. [Crossref]
- Sher T, Rottem S, Gallily R (1990) Mycoplasma capricolum membranes induce tumor necrosis factor α by a mechanism different from that of lipopolysaccharide. Cancer Immunol Immunother 31: 86-92. [Crossref]
- Sugama K, Kuwano K, Furukawa M, Himeno Y, Satoh et al. (1990) Mycoplasma induce transcription and production of tumor necrosis factor in a monocytic cell line, THP-1, by a protein kinase C-independent pathway. Infect Immun 58: 3564-3567. [Crossref]
- Kuwano K, Akashi A, Ura IM, Nishimoto M, Arai S (1993) Induction of macrophage-mediated production of tumor necrosis factor alpha by an L-form derived from Staphylococcus aureus. Infect Immun 61: 1700-1706. [Crossref]
- Shaddox L, Wiedey J, Bimstein E, Magnuson I, Salzler MC et al. (2010) Hyper-responsive Phenotype in Localized Aggressive Periodontitis. J Dent Res 89: 143-148. [Crossref]
- Lima PMA, Souza PEA, Costa JE, Gomez RS, Gollob KJ et al. (2011) Aggressive and chronic periodontitis correlate with distinct cellular sources of key immunoregulatory cytokines. J Periodontol 82: 86-95. [Crossref]