‘Brain Tissue Out’ in a Train Struck Victim: A Case Report
A B S T R A C T
Background: ‘Brain tissue out’ (BTO) is used here to describe traumatic acute extracranial cerebral herniation, an extreme manifestation of severe TBIs.
Case Description: We report a case of a 15-year-old victim of a severe head injury who was brought with acute extracranial cerebral herniation ‘brain tissue out’. We review the current literature and evidence of this exceedingly rare presentation.
Conclusion: 'Brain tissue out' is a rare form of severe head injury with a very poor prognosis. The possible catastrophic short long-term effects of this injury warrant further attention to clarify the underlying mechanisms and to identify its management guidelines.
Keywords
Severe head trauma, brain tissue herniation
Introduction
Serious traumatic brain injury (TBI) is a significant cause of death and morbidity worldwide. Penetrating traumatic brain injury is the most fatal category of TBI, with a pre-hospital mortality rate of 70-90% [1]. ‘brain tissue out’ (BTO) is used here to describe traumatic acute extracranial cerebral herniation, an extreme manifestation of severe TBIs. A traumatic acute extracranial cerebral herniation is defined here as the acute extrusion of brain parenchyma through the scalp wound at the time of the initial trauma and represents the very extreme end of the spectrum of severe TBI presentations. The documented BTO literature is scarce [2, 3]. Here, we report a case of a BTO in a train-hit patient, a rare presentation of those who survive the initial impact.
Case Description
A 15-year-old male patient was brought to the emergency department having been hit by a train. His Glasgow coma score (GCS) at admission was 5/15 (E1V1M3), brain tissue was noted exciting through a scalp wound (Figure 1) and he had 4 mm bilaterally fixed pupils as well as negative corneal response. He was resuscitated and managed in accordance with the advanced trauma life support (ATLS) guidelines.
Computed tomography (CT) scan of the brain showed an open comminuted parietal skull fracture with transcalvarial herniation of the brain parenchyma. Other findings included a depressed frontal skull fracture with supra-orbital extension, acute left-sided subdural hematoma, and a midline shift of more than 10 mm with compression of the lateral ventricles (Figure 2).
The patient was taken to surgery after initial stabilization. The surgical steps were as follows: 1) an emergency coronal skin incision, 2) left parietal decompressive craniectomy, 3) wide Dural opening performed in a cruciate fashion by extending the margins of the lacerated dura, 4) debridement of the liquified brain tissue, dural closure, using artificial dural graft 5) hemostasis and tissue closure by anatomical planes (Figures 1-4). Post-operatively, the patient was transported to the neurosurgical intensive care unit. He remained areflexic with non-reactive pupils. His condition did not change and he, unfortunately, passed away on the fifth post-operative day.
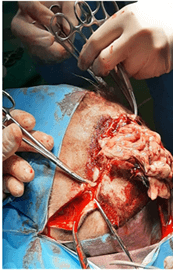
Figure 1: Brain tissue herniating out of the scalp wound.
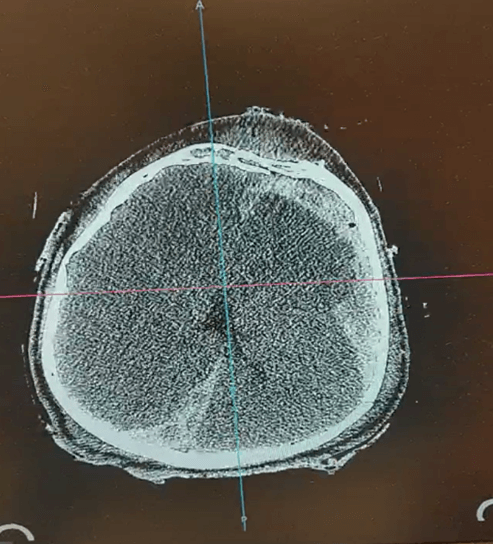
Figure 2: Axial brain CT scan showing transcalvarial brain parenchymal herniation, a left-sided frontotemporal sub-dural hematoma, bilateral compression of the lateral ventricles, effacement of the sulci, and significant midline shift.
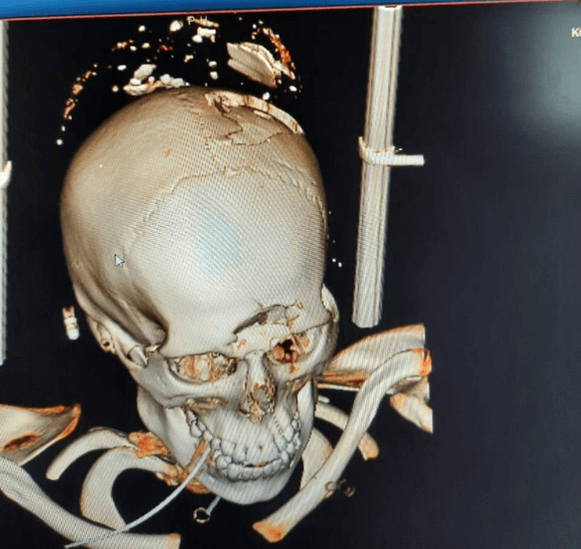
Figure 3: 3D-reconstructed CT skull, showing a skull vault avulsion fracture.
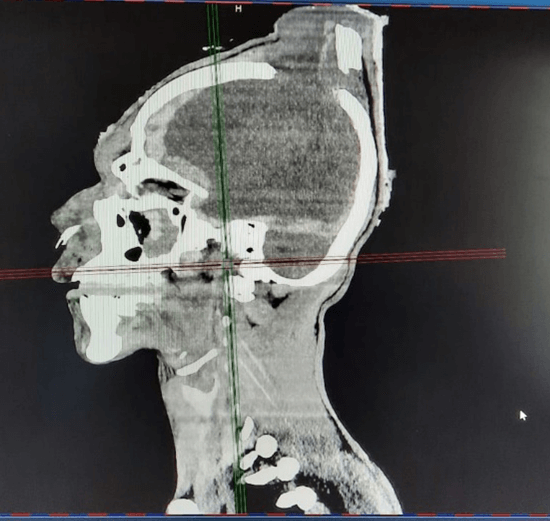
Figure 4: Sagittal CT head and neck showing a transcalvarial brain herniation through the skull vault fracture.
Discussion
Traumatic acute extracranial cerebral herniation (BTO) is an exceptionally rare and extreme presentation of severe head trauma. BTO may be caused by a variety of injury mechanisms, including penetrating, blunt, and crush injuries [3, 4]. Possible theories of the mechanism of BTO include the recurrent propagation of kinetic energy from the site of impact resulting in extrusion of the brain parenchyma through the inlet or exit wounds. The reported literature on this subject is very scarce and thus, the exact biomechanics are not completely understood [4, 5].
BTO may be categorized as post-operative and traumatic [4, 5]. Post-operative BTO is a relatively well-reported complication that occurs when the brain is herniated from a surgical wound. Traumatic BTO, on the other hand, is a very rare phenomenon that has so far been recorded only in two series. In both reports, patients suffered serious head injuries, both penetrating and blunt, caused by tear gas canisters and blast explosions, respectively.
A 100% mortality rate has been recorded in one series. In another series of 75 blast victims, the authors reported a higher 30-day mortality rate in BTO victims relative to those without brain tissue herniation, 64.1 percent versus 9%, respectively. The mean GCS was 7.4 and victims were more likely to experience complications, including seizures, cerebrospinal fluid leakage, and cerebrospinal fluid infection. Much remains to be described as far as BTO is concerned. Future research should seek to better understand its mechanisms, management, and prognostic factors.
Conclusion
'Brain tissue out' is a rare form of severe head injury with a very poor prognosis. The possible catastrophic short, long-term effects of this injury warrant further attention to clarify the underlying mechanisms and to identify its management guidelines.
Ethical Approval
None.
Consent
None.
Availability of Data and Materials
Yes.
Competing Interests
None.
Funding
None.
Acknowledgement
None.
Author Contributions
M.E.R., R.E.C., G.M., B.O.I.: Case identification and management; Z.F.A.: Manuscript drafting; S.S.H: Manuscript drafting and revision.
Abbreviation
BTO: Brain Tissue Out
GCS: Glasgow Coma Scale
Article Info
Article Type
Case Report and Review of the LiteraturePublication history
Received: Tue 14, Jun 2022Accepted: Wed 29, Jun 2022
Published: Mon 11, Jul 2022
Copyright
© 2023 Rossi Evelyn Barrientos Castillo. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.NNB.2022.02.02
Figures & Tables
References
1. Rosenfeld JV, Bell
RS, Armonda R (2015) Current concepts in penetrating and blast injury to the
central nervous system. World J Surg 39: 1352-1362. [Crossref]
2. Hoz SS, Aljuboori
ZS, Dolachee AA, Al-Sharshahi ZF, Alrawi MA et al. (2020) Fatal Penetrating
Head Injuries Caused by Projectile Tear-Gas Canisters. World Neurosurg 138:
e119-e123. [Crossref]
3. Hoz SS,
Al-Sharshahi ZF, Dolachee AA, Al-Smaysim AM, Matti WE et al. (2020)
Blast-Induced Traumatic Brain Injuries: Experience from the Deadliest Double
Suicide Bombing Attack in Iraq. World Neurosurg 145: e192-e201. [Crossref]
4. Gilardi BR, López JIM, Villegas ACH, Mora JAG, Rodríguez OCR et al. (2019) Types of Cerebral Herniation and Their Imaging Features. Radiographics 39: 1598-1610. [Crossref]
5. Sinclair AG, Scoffings DJ (2010) Imaging of the post-operative cranium. Radiographics 30: 461-482. [Crossref]