Journals
Belief in the ability to deal with an emergency situation among IDF mental health officers during a military operation
A B S T R A C T
The very nature of army mental health officers' (MHOs') work is their exposure to stressors––those experienced by those they treat, as well as those the MHOs experience directly, such as acute work-family conflict in emergency situations. This exposure is a potential source of personal distress.
Aim: To examine to what extent the MHOs of the Israeli military believe in their ability to use professional tools and effectively perform as a therapist in emergency situations.
Method: Four questionnaires were distributed in the course of a military operation (N = 87): General Self-Efficacy Scale, MHO Self-Efficacy Scale, Perceived Problem-Solving Test as a Threat Scale, and State-Trait Anxiety Inventory.
Results: Findings showed that the military tenure of MHOs was associated with their perceived ability to function as therapists (MHO self-efficacy) and with the extent to which problem-solving tasks were perceived as threatening. Longer tenure in the current military position was associated with a higher sense of general self-efficacy and a higher level of MHO self-efficacy in emergency situations. Neither gender differences, location of residence, or site of military service (near or far from the high-risk war zone) were found to be associated with the MHOs' perceived ability to function as therapists and their general self-efficacy.
Conclusion: Training MHOs in the IDF (Israel Defense Forces) during routine times, in preparation for emergency situations. is very important for functioning as a therapist. These training programs also attend to the MHOs' ability to maintain their personal resources while intervening during and after an emergency.
K E Y W O R D S
Self-efficacy, problem solving, Israeli IDF mental health officers, emergency preparedness, perceived ability to function as therapists
I N T R O D U C T I O N
Stress, crisis, and resilience are terms related directly to process of coping in an emergency situation [1-5]. An emergency is a situation that poses an immediate threat to a crucial interest (usually to life) with insufficient time to prepare for it. As the threatened interest is more crucial, and the time to prepare for dealing with it is limited, the feeling of emergency grows [4, 6]. The feeling of being under threat is increased when fear of failure is present, and when problems appear as non-resolvable [5,7,8,9]. Stress is a feeling resulting from the discrepancy between a person's need to cope with a threat and the latter's subjective conception of efficacy and resources available for active coping [10]. Intensity of stress is a function of the gap between needs and resources [11]. When the gap grows, a crisis may ensue. Crisis is a situation when orientation brakes and a feeling of uncertainty, loss of control, anxiety, and stress occur [10, 12].
A critical resource in such situations is resilience [10, 12]. Resilience refers to the ability to cope with potential loss or with actual loss and damage after their occurrence [11, 13, 14, 15]. Self-efficacy is regarded as the main foundation of resilience [13, 14]. It relates to self-esteem, locus of control, and motivation, and as such, predicts several work-related outcomes, including job attitudes, training proficiency, and job performance [16, 17]. Another critical resource in such situations is social support, an element that has been found to promote well-being and is particularly critical for coping with stress [18-21]. Social support has also been found to be an important mediator between stressful life events and mental illnesses, and thus related to resiliency [13, 22].
Individuals perceive emergency situations differently. The response to such a situation is influenced by prior experiences in similar situations, individuals' personality and strengths, and the belief in their ability to cope successfully with the threat using available knowledge and experience [4, 6]. For instance, Or: the inclination to appraise problems as a challenge, rather than as a threat, was found to be associated with cognitive flexibility and emotional regulation, and may serve as a coping resource [23] Also, it has been argued that trait anxiety is a personality disposition that describes a person's tendency to perceive situations as threatening, and hence to experience state anxiety in stressful situations [24].
Mental Health Professionals
Mental health professionals have an important role in influencing the behavior of people during emergency situations, and by providing treatment to those in need, before, during, and after occasions of crisis Over the years, due to the impact of disasters and broad combat engagements, the complexity of coping required from professionals, and the necessity to address this complexity during training and after interventions have been recognized [25-29]. As exposure to stressors and harsh scenes is inherent in the nature of the therapist's work, it necessitates a specific training focus in anticipation of dealing with emergency situations in order to maximize therapists' functioning skills and performance when needed [28, 30].
Professional training impacts both the therapist's functioning as well as those individuals in need of assistance during an emergency [31, 32]. Such training would enable professionals in various fields to intervene effectively in a variety of emergency situations [25-27]. Appropriate training would also likely lower the risk of burnout and mental illness among therapists, resulting from exposure to stressful and intensive situations during emergencies [33-35]. One of the factors found helpful in training for emergencies is the maintenance of steady and stable work during routine periods. Maximizing and persisting in routine facilitates the necessary accommodation to change in functioning as an emergency situation evolves [36].
IDF Mental Health Professionals
Mental health officers (MHOs) in the IDF comprise professionals from three fields: psychiatry (15%), psychology (25%) and social work (60%). At the time of their enlistment, these professionals are required to have graduated with a BSW degree (for social workers), a masters’ degree (for psychologists), or an M.D. (psychiatrists). Other prerequisites are expertise in clinical practice, training in trauma treatment tools and intervention skills, and experience in crisis intervention. After enlistment, psychiatrists and psychologists often enroll in internship programs in the course of their military service. Also, while serving, therapists may be entitled to pursue higher professional degrees in regular university programs.
Substantial efforts have been made to train MHOs in the IDF during routine times, in preparation for emergency situations. These training programs also attend to the MHOs' ability to maintain their personal resources while intervening during and after stressful situations, by means of preparedness, mentoring, and establishing a supportive social net [25, 27, 30, 31]. Army MHO training includes preventive clinical interventions for emotional disorders, such as acute and long-term stress reactions, to be implemented both prior and during emergency situations. This training also incorporates techniques for working with commanders on ways to recognize crisis situations and to intervene with their soldiers when needed.
In peacetime, MHOs teach and train for stress inoculation and implement psycho-educational programs for both soldiers and their commanders. This training is designed to enhance and reinforce the MHOs' resources so that they become less vulnerable or immune to the stresses characteristic of a variety of military situations. In addition, commanders are trained to instruct their soldiers to look after themselves and their peers, and, upon identifying signs of distress, soldiers are required to request the intervention of a commander or an MHO [37, 38].
While at routine times, the MHOs' practices are fairly distinct from one another, during emergency times, most MHOs are required to engage in the same type of interventions. During an emergency, emotionally-focused interventions are provided to soldiers with the goal of restoring their functioning and assisting them to return, to the greatest extent possible, to their original status. This regimen bears a strong resemblance to the classic proximity, immediacy and expectation (PIE) principles [39].
The Resilience Self- Enhancement Program is an intervention at the individual level, guided by the unit's MHO. This is a recently-designed training regimen that aims to prepare soldiers to recognize acute reactions to stress among their combat unit colleagues and to know how to help them retain their emotional strength and their coping skills, employing cognitive-behavioral methods.
Interventions on the unit level involve the commander's role in establishing and maintaining unit resilience, functioning, and mental coping in intensive situations. The commander carries out this objective in individual and/or group sessions. The technique of modified debriefing is applied to commanders and soldiers following direct exposure to danger or harsh scenes, some while engaging in their combat roles and some while assisting in rescue or treatment teams. The main goal of this intervention is for the group to achieve a fuller understanding of the different angles of the situation in order to enable all participants to process what has happened and to mutually cope with its difficulty in a manner that will help them to continue functioning and to lessen the likelihood of post-traumatic stress disorder [40, 41]. The commander's presentation to the group is monitored by the MHO behind the scenes.
While some studies have shown reduction of PTSD symptoms after using debriefing, most studies have had difficulty demonstrating clear evidence of its clinical effectiveness, and some studies even showed a worsening of stress symptoms [42-44]. However, Hawker, Durkin, and Hawker (2011) claimed that these studies are often characterized by methodological difficulties that undermine their reliability and conclusions [45]. Altogether, Hawker et al., (2011) recommended using debriefing with "professionals who had been selected for their resilience and briefed to cope with traumatic stress as an occupational hazard" (p. 461), such as soldiers and emergency service caregivers [45].
These IDF programs were designed not only to prevent future morbidity among soldiers, but also to ensure a sense of competence and belief in the MHOs' ability to treat others in distress. As such, all interventions and programs have been formulated to take into account the state of the caregivers. Professional literature has emphasized that a key element in planning interventions, is to preserve the caregivers' own resources while intervening in the course of and subsequent to an emergency [25, 30]. Therefore, professional training impacts both the functioning of the therapists and the individuals in need of assistance during an emergency [27, 31].
During emergencies, a work-family role conflict may ensue among caregivers. For example, during hurricane Katrina, only two-thirds of police officers reported for and remained on duty, and local mental health and welfare agencies also became inoperative [46]. With the civilian home front directly and continuously being bombarded by rocket and mortar fire, MHOs are often required to spend extended periods away from home, while constantly apprehensive regarding their family’s safety.
Bar-Tal, Lurie, and Glick (1994) examined the effect of gender on stress among Israeli soldiers during the Gulf War [47]. They found that stress had stronger negative impact on females than on males, and, while females were more likely to perceive their own coping as effective, it had less positive effect on them than males' coping behavior had on themselves. These gender differences may be explained by different coping strategies, specifically, problem-focused versus "emotion-focused for men and women, respectively. It has been argued that men tend to underestimate the magnitude of stressful events and are likely to engage in distracting activities. Different gender roles and definitions of feminine and "masculine behaviors in society may also affect response to stressful situations. Lastly, men and women may differ in their willingness to report their reactions [48].
Pillar of Defense Operation
On November 14-21, 2012, in response to the major terror escalation from the Gaza Strip, Israel launched Operation Pillar of Defense. During the operation, which began with the killing of the Hamas' military wing chief in Gaza, about 1,700 rockets and over 50 mortar shells were fired into Israel from the Gaza Strip. Advanced anti-air and anti-tank rockets were also fired into Israel. Following eight days of fighting, a ceasefire was announced on November 21, 2012 [49]. Starting the first day of the operation, and through the entire period, MHOs conducted intensive interventions, primarily aimed at reducing acute stress symptoms.
The Current Study
Much has been reported in the literature regarding coping mechanisms during natural and man-made disasters, especially after 9/11, but only little has related to the preparation of resilient and functioning mental health professionals for emergency situations [40]. The current research sought to determine to what extent MHOs believe in their ability to act effectively in an emergency. Additional aims were to assess MHOs' belief in the professional tools available to them, as well as their belief in the effectiveness of their professional supervision and their social support net. To do so, a questionnaire designed for the current study was used to assess participants’ self-efficacy as therapists in the Israeli military setting.
It was hypothesized that females MHOs would show less self-efficacy and more threat perception and state anxiety than would males, due to gender differences in coping strategies and cultural influence [47, 48]. As different military occupations comprise different training and knowledge, professions differences on the study variables were also expected. Greater residential and service proximity to the war zone was expected to be associated with greater stress and less accessible to be of assistance to others.46 Consequently, these variables were expected to be negatively associated with self-efficacy and challenge perception. Rank, overall military tenure, and current military position tenure were expected to be positively associated with self-efficacy and challenge perception, in that authority, available knowledge, and experience may serve as a buffer against stress, and boost feelings of self-competency [4, 6]. Lastly, state anxiety and perceiving problems as a challenge or threat were hypothesized to mediate the association between general self-efficacy and MHO self-efficacy. MHO self-efficacy, in contrast to general self-efficacy, is expected to take into account the specific characteristics of being a therapist in dangerous and stressful situations. Therefore, anxiety regulation and the ability to cognitively construct threats as challenges are especially important in the military sphere.
The study of mental caregivers' resilience and general functioning is critical in conflict areas. To the best of our knowledge, this is the first effort to systematically assess these issues
Methods
Participants
This survey was conducted during the Pillar of Defense operation of November 2012. Two hundred eight MHOs participated in this survey, of whom 87 completed the full questionnaire (33 men [38%] and 54 women [62%]). All participants were MHOs on active duty in the IDF. Fifteen participants (17.2%) completed the questionnaire during the first day of the eight-day operation, 13 (15%) during the second and third days, 23 (26.4%) during the fourth and fifth days, and the remaining 36 (41.4%) responded during the remaining days. The participants were assured of the anonymity of the questionnaires.
Among the MHO participants, 21 (24.2%) both lived and served within the high-risk missile zone (within approximately 40 kilometers from the Gaza Strip border), with both they and their families being directly subject to continued missile strikes. Twelve participants (13.8%) served within the high-risk zone, with their close family relatively safe, residing beyond the high-risk zone; 66 (75.8%) lived beyond the high-risk zone, and 75 (86.2) served beyond the high-risk zone. All were keenly aware of soldiers, relatives, and friends living or serving within Gaza or within the high-risk zone. The sample is representative of the MHO sample in the Israeli army in age, gender, marital status, profession, rank, and tenure. Participant characteristics are presented in Table 1.
Procedures
Self-administered questionnaires were sent by E-mail to all the MHOs on the first day of the Pillar of Defense operation (November 2012). Only those who agreed to complete the questionnaires received them and participated in the study. Eighty-seven MHOs out of a total of 150 responded. The participants were assured that the questionnaires would be used for research purposes only.
Materials
The General Self-Efficacy Scale (GSE). This scale was designed to assess a general sense of self-efficacy, aiming to predict coping with daily hassles as well as adaptation after experiencing stressful life events [50]. Item examples were: I can always manage to solve difficult problems if I try hard enough, and, When I am confronted with a problem, I can usually find several solutions. The scale comprises 10 statements, with participants requested to respond on a 4-point Likert-type scale, ranging from: 1(not at all true) (1), to 4 (exactly true). The questionnaire was found to have good internal consistency and reliability. Cronbach's alpha in our study was α = .97.
MHO Self-Efficacy Scale. This questionnaire was created especially for this study to assess participants’ self-efficacy as therapists in the 'military conflict setting. The questionnaire was designed three days prior to the start of the Pillar of Defense operation of November 2012. The questionnaire's items were grounded in the accumulated knowledge regarding the functioning and perceptions of personnel in the military mental health departments in emergency situations. Over the past decade, similar questions have been posed globally, in the wake of catastrophic events or disasters [25,28,29,45].
The participants of this study were MHOs on active duty in the IDF, and they completed the questionnaire during the first day to the middle of second week of the operation. This specific scale was required in light of this study's focus on a very specific population performing its professional tasks in a unique setting. The 10-item questionnaire included statements such as: I feel prepared for a long stay away from home; I am competent in intervention techniques for crisis and stress that will help me cope with situations with solders and commanders; I have with whom to consult professionally when needed; I feel confident in the interventions techniques I have mastered and in my ability to intervene with others, even while my family is under threat. To examine its construct validity, we conducted a confirmatory factor analysis (CFA) using MPlus 6.1 structural equation modeling packet [51]. The CFA had excellent fit to the observed data, χ2(33) = 44.02, p = .10, CFI = .97, TLI = .95, RMSEA = .06 [90% CI: .00, .11], SRMR = .07. Average loading of the items was 0.62 (Cronbach’s α = .84). Accordingly, we calculated a mean MHO self-efficacy score for each participant.
Perceiving Problem–Solving Task as a Threat scale. This 14-item questionnaire was designed to examine individuals’ belief in their ability to solve interpersonal problems and measures the perceptions of people about their attitudes and behaviors when trying to resolve interpersonal problems [23]. The items included statements such as: Before performing a task, I feel curious; Before performing a task, I feel threatened, where seven items measured the perception of the problem as a threat and seven items measured the perception of the problem as a challenge. The participants responded to the questionnaire on a 5-point Likert-type scale, ranging from 1 (strongly disagree) to 5 (definitely agree). Cronbach's alpha in our study was α = .87.
State-Trait Anxiety Inventory (STAI). The STAI measures two types of anxiety: state anxiety (anxiety about an event) and trait anxiety (anxiety level as a personal characteristic). The 40-item questionnaire was presented on a 4-point Likert-type scale, ranging from 1 (almost never) to 4 (almost always). State anxiety items included: I am tense; I am worried; I feel calm; I feel secure. Higher scores are positively correlated with higher levels of anxiety [52]. Cronbach's alpha in our study was α = .87. As this study has focused on reactive anxiety due to environmental and circumstantial factors, we used only the state anxiety scale.
Demographic questionnaire. Participants were asked to indicate their age, gender, marital status, profession, military rank, general home residence location, locale of active military service, overall military tenure, and tenure of current military role. Since soldiers are awarded rank after a certain number of years of service, various roles, professional experience, and outstanding evaluations, we classified the overall military tenure into three categories: 0-3, 4-5, and 6 and above years. As most MHOs serve 2-4 years in the same military position, and in order to express the accommodation process to a new professional environment, we classified the current military position tenure into three categories: to up to one year, 1-2 years, and 3 and above years
Data Analysis
Statistical analyses were conducted using SPSS (Version 21.0 for Windows). A 95% (p value < .05) significance level was adopted. Pearson's correlation matrix was used to show the relationships between the variables measured. One-way ANOVA analyses were used in order to assess the differences between the categorical independent variables with three or more groups. In the case of heterogeneous variance, we used the Brown-Forsythe adjustment. To examine the source of differences between the groups, we employed either the Bonferroni post-hoc analysis (in case of homogenous variance) or the Tamhane post-hoc analysis (in case of heterogeneous variance). Independent samples t tests were used in order to assess the differences between the categorical independent variables with two groups.
Finally, we employed Hayes’s (2009)multiple-step mediation methodology to examine whether therapists' perception of problem solving (threat and/or challenge) and state anxiety mediated the link between their self-efficacy and perceived ability to function as therapists. Significance of the indirect paths was tested using accelerated bias-corrected bootstrap analyses [53].
Ethics Approval
The study was approved by the IDF Human Research Review Board. In addition, the study recruitment team did not have any relationship with the participants' units and all participants were informed they could discontinue the interview at any time.
Tables
Table 1: Study Population (N = 87)
|
% |
N |
|
|
38.0 62.0 |
33 54 |
Gender: Male Female |
|
24.1 37.9 24.1 13.8 |
21 33 21 12 |
Age: 25-30 30-35 35-40 >40 |
|
51.8 12.6 35.6 |
45 11 31 |
Overall military tenure (in years): 0-3 4-5 >6 |
|
|
|
Tenure in current military role (in years) |
|
41.2 25.6 33.2 |
36 22 29 |
Up to 1 year 1-2 3+ |
|
8.3 58.5 33.2 |
7 51 29 |
Rank: Lieutenant Captain Major |
|
27.6 72.4 |
24 63 |
Marital status: Single Married |
|
24.2 75.8 |
21 66 |
Residence location: Within high-risk zone* Beyond high-risk zone |
|
13.8 86.2 |
12 75 |
Service locale: Within high-risk zone* Beyond high-risk zone |
Note: *Lived or served (mostly) within the 40-kilometer range from the Gaza Strip, thus being exposed to continuous missile strikes, as were their families.
Table 2: Differences Between Gender and Military Professions in the Main Study Measures
|
d |
t(85) |
Women (n = 54) |
Men (n = 33) |
Gender |
|||
|
SD |
M |
SD |
M |
||||
|
.25 |
1.16 |
4.67 |
33.07 |
3.23 |
34.15 |
General self-efficacy |
|
|
.21 |
-.96 |
4.99 |
14.57 |
4.65 |
13.55 |
Threat1 |
|
|
.13 |
-.59 |
4.31 |
24.20 |
6.75 |
23.42 |
Challenge1 |
|
|
.31 |
-1.42 |
11.43 |
38.26 |
7.76 |
35.33 |
Trait anxiety |
|
|
.37 |
1.71 |
5.73 |
29.22 |
4.36 |
31.21 |
(MHO self-efficacy 2 |
|
|
d |
t(85) |
Psychologists (n = 25) |
Social workers (n = 61) |
Professions |
|||
|
SD |
M |
SD |
M |
||||
|
.23 |
1.08 |
5.35 |
32.64 |
3.61 |
33.90 |
General self-efficacy |
|
|
.24 |
1.12 |
3.56 |
13.32 |
5.24 |
14.41 |
Threat1 |
|
|
.10 |
-.44 |
5.78 |
24.80 |
5.23 |
23.72 |
Challenge1 |
|
|
.02 |
.07 |
9.16 |
36.92 |
10.74 |
37.08 |
State anxiety |
|
|
.25 |
1.16 |
5.53 |
29.00 |
5.22 |
30.46 |
MHO2 |
|
Note: * p < .05, ** p < .01. 1Perception of problem-solving task. 2 MHOs' (army mental health officers')
Table 3: Differences between Participants' Residence and Service Locations in the Main Study measures (N=87)
|
F(2, 84) |
Other (n = 25) |
Center of Israel (n = 41) |
High-risk zone (n = 21) |
Residence Location |
||||||
|
SD |
M |
SD |
M |
SD |
M |
|||||
|
.02 |
.71 |
4.24 |
33.04 |
3.77 |
34.05 |
4.97 |
32.90 |
General self- efficacy |
||
|
.002 |
.08 |
4.08 |
13.88 |
5.44 |
14.24 |
4.73 |
14.43 |
Threat1 |
||
|
.06 |
2.83 |
4.34 |
22.24 |
5.74 |
25.27 |
5.14 |
23.24 |
Challenge1 |
||
|
.02 |
.88 |
10.76 |
37.12 |
10.76 |
35.93 |
9.33 |
39.57 |
state anxiety |
||
|
.03 |
1.28 |
4.86 |
28.64 |
4.86 |
30.24 |
6.60 |
31.05 |
MHOs' self-efficacy 2 |
||
|
η2 |
F(2, 84) |
Other (n = 23) |
Center of Israel (n = 43) |
High-risk zone (n = 21) |
Work Location |
|||||
|
SD |
M |
SD |
M |
SD |
M |
|||||
|
.002 |
.10 |
4.16 |
33.17 |
3.77 |
33.65 |
5.32 |
33.48 |
General self- efficacy |
||
|
.01 |
.39 |
4.31 |
14.39 |
4.79 |
13.74 |
5.68 |
14.86 |
Threat1 |
||
|
.05 |
2.37 |
4.00 |
22.17 |
5.79 |
24.00 |
5.32 |
25.62 |
Challenge1 |
||
|
.003 |
.11 |
10.12 |
36.70 |
10.19 |
36.95 |
10.94 |
38.05 |
State anxiety |
||
|
.04 |
1.92 |
4.62 |
28.35 |
4.77 |
30.14 |
6.70 |
31.43 |
MHOs' self- efficacy 2 |
||
|
t |
|
|
|
|
|
|
|
|
||
Note: *p < .05, **p < .01. 1Perception of problem-solving task. 2 MHOs' (army mental health officers')
Table 4: Differences Between Overall Military Tenure Groups in the Main Study Measures (N = 87)
|
η2 |
F(2, 84) |
6+ years (n = 31) |
4-5 years (n = 11) |
0-3 years (n = 45) |
Overall military tenure |
|||
|
SD |
M |
SD |
M |
SD |
M |
|
||
|
.004 |
.18 |
3.90 |
33.74 |
3.60 |
33.82 |
4.59 |
33.22 |
General self-efficacy |
|
.07 |
3.22* |
4.33 |
12.45b |
5.13 |
15.00 |
4.91 |
15.18a |
Threat1 |
|
.05 |
2.96 |
6.83 |
22.42 |
2.46 |
23.36 |
4.43 |
25.07 |
Challenge1 |
|
.01 |
.35 |
9.05 |
35.94 |
11.50 |
37.27 |
10.85 |
37.96 |
State anxiety |
|
.09 |
4.26* |
5.16 |
32.13b |
4.68 |
28.55 |
5.20 |
28.84a |
MHO2 self-efficacy |
Note: * p < .05. Means with different superscript letters are significantly different at p < .05. 1 Perception of problem-solving task. 2 MHOs (army mental health officers)
Table 5: Differences between Current Military position tenure groups in the main study measures (N = 87)
|
η2 |
F(2, 84) |
3+ years (n = 29) |
1-2 years (n = 22) |
Up to 1 year (n = 36) |
Current military position tenure |
|||||
|
SD |
M |
SD |
M |
SD |
M |
|
||||
|
.09 |
4.27* |
3.69 |
35.28b |
3.58 |
32.68 |
4.56 |
32.53a |
Self-efficacy |
||
|
.04 |
1.68 |
4.42 |
13.52 |
4.53 |
13.22 |
5.29 |
15.31 |
Threat1 |
||
|
.03 |
1.53 |
6.24 |
22.69 |
4.05 |
25.23 |
5.18 |
24.08 |
Challenge1 |
||
|
.06 |
2.82 |
8.38 |
34.26 |
11.98 |
41.27 |
9.97 |
36.67 |
State anxiety |
||
|
.11 |
5.35** |
3.97 |
32.28b |
5.69 |
29.59 |
5.44 |
28.28a |
MHO2 self-efficacy |
||
Note: * p < .05, ** p < .01. Means with different superscript letters are significantly different at p < .05. 1Problem-solving task. 2 MHOs' (army mental health officers'
Table 6: Standarised Coefficents in the Adjusted Model and Fit Indeces in Multiple Group Pathway Analysis (df=17)
|
d |
t(85) |
Major and above (n = 26) |
Captain and below (n = 58) |
Military rank |
||
|
SD |
M |
SD |
M |
|
||
|
.23 |
-1.05 |
3.95 |
34.15 |
4.39 |
33.10 |
Self-efficacy |
|
.67 |
3.09** |
4.13 |
11.73 |
4.90 |
15.14 |
Threat1 |
|
.46 |
2.10* |
6.43 |
22.31 |
4.57 |
24.78 |
Challenge1 |
|
.34 |
1.59 |
9.29 |
34.65 |
10.66 |
38.50 |
State anxiety |
|
.68 |
-3.13** |
4.10 |
32.65 |
5.52 |
28.86 |
MHO2 self-efficacy |
Note: * p < .05, ** p < .01. 1Perception of problem-solving task. 2 MHOs' (army mental health officers)
Table 7: Unstandardized Regression Coefficients and Bootstrap Confidence Intervals for Predicting the Perceived Ability to Function as a Therapist by Self-efficacy Through Perception of Problem-Solving and State Anxiety
|
MHO self-efficacy |
|
|
.60*** |
Direct effect of general self-efficacy |
|
(-.01, .31) |
Indirect via problem-solving task as a threat |
|
(.01, .15)* |
Indirect via problem-solving task as a challenge |
|
(-.04, .20) |
Indirect via State anxiety |
|
(-.04, .09) |
Indirect via problem-solving task as a threat and state anxiety |
|
(-.01, .21) |
Indirect via problem-solving task as a challenge and state anxiety |
Note: * p < .05, ** p < .01. Confidence intervals not including 0 (null association) are significant.
R e s u l t s
To examine whether gender and profession differ in the main study measures, we employed a series of independent samples t tests, in which those variables served as the independent variable, and the main study measures as the dependent variables. Means, standard deviations, statistics, and effect sizes are presented in Table 2. The analyses indicated that men and women did not significantly differ in any of the study measures. Similarly, the analyses indicated that social workers and psychologists were not significantly different in any of the study measures.
To examine whether residence location (three categories: within the high-risk zone, center of Israel, and other) and service location (within the high-risk zone, center of Israel, and other) is associated with the main study variables, we conducted a series of one-way analysis of variance (ANOVA). Residence location and service location served as the independent variable, and the main study measures as the dependent variables. In the case of heterogeneous variance, we used the Brown-Forsythe adjustment. To examine the source of differences between groups of various tenures we employed either the Bonferroni post-hoc analysis (in the case of homogenous variance) or the Tamhane post-hoc analysis (in the case of heterogeneous variance). Means, standard deviations, statistics, and effect sizes are presented in Table 3. The analyses indicated that participants in the various service locations did not significantly different in any of the study measures, nor were there any significant differences on the study measures among those living in the various resident location categories.
To examine whether overall military tenure was associated with the main study measures, we conducted a series of one-way analysis of variance (ANOVA), in which overall military tenure served as the independent variable, and the main study measures as the dependent measures. In case of heterogeneous variance, we used the Brown-Forsythe adjustment. To examine the source of differences between the tenure groups we employed either the Bonferroni post-hoc analysis (in case of homogenous variance) or the Tamhane post-hoc analysis (in case of heterogeneous variance). Means, standard deviations, statistics, and effect sizes are presented in Table 4. we found that group with a professional tenure of more than 6 years perceived problem-solving tasks as less threatening and perceived their ability to function as therapists as higher than the 0-3-year tenure group. Nonetheless, tenure greater than 6 years did not significantly enhance self-efficacy. The differences between tenure groups in the main study measures are presented in Table 4.
Findings also show that therapists with a rank of major or above perceived their ability to function as a therapist higher than participants with a rank of captain or below (p < .01). They perceived problem-solving tasks as less threatening (p < .01), but also as less challenging than the lower-ranked group (p < .05). Differences between ranks in the main study measures are presented in Table 6
Next, we examined whether therapists' perception of problem solving (threat and/or challenge) and state anxiety mediated the link between their general self-efficacy and MHO self-efficacy. Specifically, we examined
(1) whether general self-efficacy directly affected MHO self-efficacy, controlling for perception of problem-solving and state anxiety,
(2) whether general self-efficacy indirectly affected perceived ability to function as therapists (MHO self-efficacy) via perception of problem-solving,
(3) whether general self-efficacy indirectly affected perceived ability to function as therapists via state anxiety, and
(4) whether general self-efficacy indirectly affected perceived ability to function as therapists (MHO self-efficacy) via (a) perception of problem-solving, and in turn (b) state anxiety (i.e., a 2-step mediational process). Unstandardized coefficients and bootstrap solutions are presented in Table 7 (see also Figure 1).
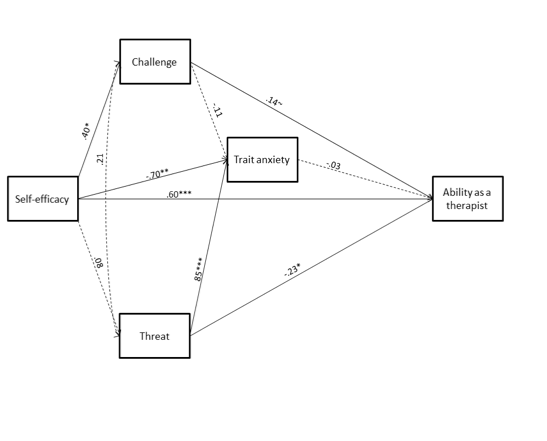
Figure 1: Indirect paths between problem-solving, trait anxiety, and self-efficacy, and ability to function as therapist in emergency situations (MHO self-efficacy).
As can be seen in Table 7 and Figure 1, the multiple-step mediation model revealed that the level of general self-efficacy indirectly affected the participants' belief in their ability to function as therapists (MHO self-efficacy) via their perception of problem solving as challenging: the higher the general self-efficacy, the higher the perception of challenge, and in turn, the higher the perception of their ability to function as therapists (MHO self-efficacy). The other mediation paths were not significant. Overall, the model explained 46.01% of the variance in therapists' perception of their ability to function as therapists, F (4, 82) = 17.47, p < .0001.
Finally, as can be seen in Figure 1, findings indicated that therapists' general self-efficacy indirectly affected their perceived ability to function as therapists (MHO self-efficacy) via their perception of problem solving as challenging, and that their perception of problem solving as challenging enhances the effect of MHO self-efficacy.
D i s c u s s i o n
The current study is the first conducted in the IDF Mental Health Department addressing the issues of the extent to which mental health officers believe in their ability to perform in an emergency, the extent to which they belief in available professional tools and in their mentoring resources. As expected, we found that participants with an overall military tenure of more than six years perceived problem-solving tasks as less threatening and perceived their ability to function as therapists (MHOs) as higher (p < .05) than those with a tenure of up to five years. Nonetheless, it was surprising to find that a tenure of more than six years did not significantly enhance MHO self-efficacy.
We also sought to examine in the current study whether tenure at the current military position and rank would contribute to general self-efficacy or to the MHOs’ belief in their ability to function as a therapist in emergencies. Differences were related to the overall military tenure, tenure at the current military position and rank. The tenure groups with respect to the current position differed in their general self-efficacy, and in their perceived ability to function as a therapist in an emergency setting (MHO self-efficacy). The group with a tenure of more than two years in the current position reported higher general self-efficacy (p < .05) and perceived a greater ability to function as therapists in an emergency setting (p < .01) than did the participants serving in their first year in the current military position. Indeed, this finding is not surprising. Since the typical duration of a military position ranges between two-four years, it is reasonable to assume that novice trainees are unlikely to demonstrate high levels of MHO self-efficacy in their first year.
The multiple-step mediation models revealed that general self-efficacy indirectly affected MHOs' perceived ability to function as therapists in an emergency setting (MHO self-efficacy) via their perception of problem solving as challenging: the greater the general self-efficacy, the greater the perception of challenge, and in turn, the higher level the perception of their ability to function as therapists (MHO self-efficacy) in emergency situations. The other mediation paths were not significant. Overall, the model explained 46.01% of the variance in therapists' perception of their ability to function as therapists.
The findings in the present study are supported by reports stating the importance of emergency training to be based on the workers’ and the unit's on-going and stable preparedness during routine times.31,32,27 The most surprising findings in this study, and in stark contrast to our hypotheses, were that neither the therapists' gender nor their own home being located in the high-risk zone comprised significant factors in any of the study variables. Furthermore, the MHOs' sense of general self-efficacy and belief in their ability to function as therapists were not affected by gender and residence location.
These findings contrast with the professional disaster literature (e.g., Hurricane Katrina; Indonesia in the 2004 tsunami disaster), where a high percentage of rescue personnel were unable to function effectively, due to work-family conflicts, when their family members were at risk [46]. These curious findings may be explained by what is known about adaptive coping strategies with stress. As men tend to use more problem-focused strategy, engage in distracting activities, and comply with the masculine gender role, they are more resilient to stress [47, 48]. Similarly, as military therapists continuously engage in training and preparations for emergencies, a more problem-focused strategy may be encouraged, in contrast to the less adaptive emotion-focused strategy. Also, the emergency situation may serve as a distracting activity from maladaptive cognitions and emotions. Along with the male-dominated military environment, those tendencies may blur the gender differences found in previous studies and thus contribute to similar coping strategies and overall functioning. Another possible explanation is the recognition that Israel’s home front has continuously been exposed to danger for decades, creating a strong linkage between the battle front and the home front. This is unlikely to be the case in incidents of natural disasters or other home-front distressful events, as they are more likely to be sudden and unanticipated. Thus, Israeli MHOs are more conscious of the prospect of such work-family conflict and have time to mentally prepare themselves and their family to function under fire in wartime.
The innovation in this study is related to the MHOs' perceived self-efficacy as therapists in an emergency situation, a measure designed specifically for this study. In light of the current findings, one could suggest that in order to better prepare the MHOs for their future missions, the army should consider conducting an advanced on-the-job training (OJT) program at the start of an armed conflict for those with the following profile: those with up to four years of tenure in military service and up to two years in the military position. The preparedness of those with more than six years' tenure must be enhanced, in order to maximize their performance, in order to function better. This is true regardless of the particular MHO profession (social workers or clinical psychologists) or gender. A possible explanation for this lack of differentiation lies in the fact that during wartime, all IDF mental health professionals, with no distinction of gender or specific profession are tasked with performing the same interventions: all treat cases of stress reaction, and all work with the commanders. Future research would do well to concentrate on validating MHOs' perceived self-efficacy as therapists in that used in this study.
Several limitations characterized the current study. The sample size was relatively small. This affected the statistical analysis and the small total population of MHOs did not enable more widespread testing. The data analysis section indicates that multiple analyses, including multiple t tests, were carried out. This increases the chance for a Type I error.
Nonetheless, the participants examined in this study reflect a representative sample of actual MHOs among the Israeli military caregiver’s population. The MHO Self-Efficacy Scale requires more development, such as administering it on larger samples in order to substantiate it as a tool relevant for other frameworks that employ therapists in emergency situations. Further investigations should incorporate actual supervisor evaluations for performance in emergency situations to supplement and corroborate the examined self-efficacy measures among MHO personnel.
As a further limitation, it may be that MHO participants completing the surveys during the initial days of the operation reported greater resiliency than those who completed them during the final days of the operation. However, the participants (MHOs) completed the questionnaire during the first day to the middle of second week of the operation (Total of 8 days of military operation).
The role of mental health care givers during military combat situations, as well as during natural disasters or terrorist catastrophes, is of great importance. Training during routine times is important for job functioning as well as for self-efficacy. Further research is needed to better understand what would facilitate their best performance, as therapists having confidence in their ability, even when they and/or their families are in danger. Future research should examine the factors that promote and maintain resiliency among these individuals.
Article Info
Article Type
Research ArticlePublication history
Received: Sat 14, Apr 2018Accepted: Mon 30, Apr 2018
Published: Sun 06, May 2018
Copyright
© 2023 Leah Shelef. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.10xx/j.PDR.2018.10.002
Author Info
Corresponding Author
Leah ShelefPsychology Branch, Israel Air Force, Ramat-Gan, Israel
Figures & Tables
Table 1: Study Population (N = 87)
|
% |
N |
|
|
38.0 62.0 |
33 54 |
Gender: Male Female |
|
24.1 37.9 24.1 13.8 |
21 33 21 12 |
Age: 25-30 30-35 35-40 >40 |
|
51.8 12.6 35.6 |
45 11 31 |
Overall military tenure (in years): 0-3 4-5 >6 |
|
|
|
Tenure in current military role (in years) |
|
41.2 25.6 33.2 |
36 22 29 |
Up to 1 year 1-2 3+ |
|
8.3 58.5 33.2 |
7 51 29 |
Rank: Lieutenant Captain Major |
|
27.6 72.4 |
24 63 |
Marital status: Single Married |
|
24.2 75.8 |
21 66 |
Residence location: Within high-risk zone* Beyond high-risk zone |
|
13.8 86.2 |
12 75 |
Service locale: Within high-risk zone* Beyond high-risk zone |
Note: *Lived or served (mostly) within the 40-kilometer range from the Gaza Strip, thus being exposed to continuous missile strikes, as were their families.
Table 2: Differences Between Gender and Military Professions in the Main Study Measures
|
d |
t(85) |
Women (n = 54) |
Men (n = 33) |
Gender |
|||
|
SD |
M |
SD |
M |
||||
|
.25 |
1.16 |
4.67 |
33.07 |
3.23 |
34.15 |
General self-efficacy |
|
|
.21 |
-.96 |
4.99 |
14.57 |
4.65 |
13.55 |
Threat1 |
|
|
.13 |
-.59 |
4.31 |
24.20 |
6.75 |
23.42 |
Challenge1 |
|
|
.31 |
-1.42 |
11.43 |
38.26 |
7.76 |
35.33 |
Trait anxiety |
|
|
.37 |
1.71 |
5.73 |
29.22 |
4.36 |
31.21 |
(MHO self-efficacy 2 |
|
|
d |
t(85) |
Psychologists (n = 25) |
Social workers (n = 61) |
Professions |
|||
|
SD |
M |
SD |
M |
||||
|
.23 |
1.08 |
5.35 |
32.64 |
3.61 |
33.90 |
General self-efficacy |
|
|
.24 |
1.12 |
3.56 |
13.32 |
5.24 |
14.41 |
Threat1 |
|
|
.10 |
-.44 |
5.78 |
24.80 |
5.23 |
23.72 |
Challenge1 |
|
|
.02 |
.07 |
9.16 |
36.92 |
10.74 |
37.08 |
State anxiety |
|
|
.25 |
1.16 |
5.53 |
29.00 |
5.22 |
30.46 |
MHO2 |
|
Note: * p < .05, ** p < .01. 1Perception of problem-solving task. 2 MHOs' (army mental health officers')
Table 3: Differences between Participants' Residence and Service Locations in the Main Study measures (N=87)
|
F(2, 84) |
Other (n = 25) |
Center of Israel (n = 41) |
High-risk zone (n = 21) |
Residence Location |
||||||
|
SD |
M |
SD |
M |
SD |
M |
|||||
|
.02 |
.71 |
4.24 |
33.04 |
3.77 |
34.05 |
4.97 |
32.90 |
General self- efficacy |
||
|
.002 |
.08 |
4.08 |
13.88 |
5.44 |
14.24 |
4.73 |
14.43 |
Threat1 |
||
|
.06 |
2.83 |
4.34 |
22.24 |
5.74 |
25.27 |
5.14 |
23.24 |
Challenge1 |
||
|
.02 |
.88 |
10.76 |
37.12 |
10.76 |
35.93 |
9.33 |
39.57 |
state anxiety |
||
|
.03 |
1.28 |
4.86 |
28.64 |
4.86 |
30.24 |
6.60 |
31.05 |
MHOs' self-efficacy 2 |
||
|
η2 |
F(2, 84) |
Other (n = 23) |
Center of Israel (n = 43) |
High-risk zone (n = 21) |
Work Location |
|||||
|
SD |
M |
SD |
M |
SD |
M |
|||||
|
.002 |
.10 |
4.16 |
33.17 |
3.77 |
33.65 |
5.32 |
33.48 |
General self- efficacy |
||
|
.01 |
.39 |
4.31 |
14.39 |
4.79 |
13.74 |
5.68 |
14.86 |
Threat1 |
||
|
.05 |
2.37 |
4.00 |
22.17 |
5.79 |
24.00 |
5.32 |
25.62 |
Challenge1 |
||
|
.003 |
.11 |
10.12 |
36.70 |
10.19 |
36.95 |
10.94 |
38.05 |
State anxiety |
||
|
.04 |
1.92 |
4.62 |
28.35 |
4.77 |
30.14 |
6.70 |
31.43 |
MHOs' self- efficacy 2 |
||
|
t |
|
|
|
|
|
|
|
|
||
Note: *p < .05, **p < .01. 1Perception of problem-solving task. 2 MHOs' (army mental health officers')
Table 4: Differences Between Overall Military Tenure Groups in the Main Study Measures (N = 87)
|
η2 |
F(2, 84) |
6+ years (n = 31) |
4-5 years (n = 11) |
0-3 years (n = 45) |
Overall military tenure |
|||
|
SD |
M |
SD |
M |
SD |
M |
|
||
|
.004 |
.18 |
3.90 |
33.74 |
3.60 |
33.82 |
4.59 |
33.22 |
General self-efficacy |
|
.07 |
3.22* |
4.33 |
12.45b |
5.13 |
15.00 |
4.91 |
15.18a |
Threat1 |
|
.05 |
2.96 |
6.83 |
22.42 |
2.46 |
23.36 |
4.43 |
25.07 |
Challenge1 |
|
.01 |
.35 |
9.05 |
35.94 |
11.50 |
37.27 |
10.85 |
37.96 |
State anxiety |
|
.09 |
4.26* |
5.16 |
32.13b |
4.68 |
28.55 |
5.20 |
28.84a |
MHO2 self-efficacy |
Note: * p < .05. Means with different superscript letters are significantly different at p < .05. 1 Perception of problem-solving task. 2 MHOs (army mental health officers)
Table 5: Differences between Current Military position tenure groups in the main study measures (N = 87)
|
η2 |
F(2, 84) |
3+ years (n = 29) |
1-2 years (n = 22) |
Up to 1 year (n = 36) |
Current military position tenure |
|||||
|
SD |
M |
SD |
M |
SD |
M |
|
||||
|
.09 |
4.27* |
3.69 |
35.28b |
3.58 |
32.68 |
4.56 |
32.53a |
Self-efficacy |
||
|
.04 |
1.68 |
4.42 |
13.52 |
4.53 |
13.22 |
5.29 |
15.31 |
Threat1 |
||
|
.03 |
1.53 |
6.24 |
22.69 |
4.05 |
25.23 |
5.18 |
24.08 |
Challenge1 |
||
|
.06 |
2.82 |
8.38 |
34.26 |
11.98 |
41.27 |
9.97 |
36.67 |
State anxiety |
||
|
.11 |
5.35** |
3.97 |
32.28b |
5.69 |
29.59 |
5.44 |
28.28a |
MHO2 self-efficacy |
||
Note: * p < .05, ** p < .01. Means with different superscript letters are significantly different at p < .05. 1Problem-solving task. 2 MHOs' (army mental health officers'
Table 6: Standarised Coefficents in the Adjusted Model and Fit Indeces in Multiple Group Pathway Analysis (df=17)
|
d |
t(85) |
Major and above (n = 26) |
Captain and below (n = 58) |
Military rank |
||
|
SD |
M |
SD |
M |
|
||
|
.23 |
-1.05 |
3.95 |
34.15 |
4.39 |
33.10 |
Self-efficacy |
|
.67 |
3.09** |
4.13 |
11.73 |
4.90 |
15.14 |
Threat1 |
|
.46 |
2.10* |
6.43 |
22.31 |
4.57 |
24.78 |
Challenge1 |
|
.34 |
1.59 |
9.29 |
34.65 |
10.66 |
38.50 |
State anxiety |
|
.68 |
-3.13** |
4.10 |
32.65 |
5.52 |
28.86 |
MHO2 self-efficacy |
Note: * p < .05, ** p < .01. 1Perception of problem-solving task. 2 MHOs' (army mental health officers)
Table 7: Unstandardized Regression Coefficients and Bootstrap Confidence Intervals for Predicting the Perceived Ability to Function as a Therapist by Self-efficacy Through Perception of Problem-Solving and State Anxiety
|
MHO self-efficacy |
|
|
.60*** |
Direct effect of general self-efficacy |
|
(-.01, .31) |
Indirect via problem-solving task as a threat |
|
(.01, .15)* |
Indirect via problem-solving task as a challenge |
|
(-.04, .20) |
Indirect via State anxiety |
|
(-.04, .09) |
Indirect via problem-solving task as a threat and state anxiety |
|
(-.01, .21) |
Indirect via problem-solving task as a challenge and state anxiety |
Note: * p < .05, ** p < .01. Confidence intervals not including 0 (null association) are significant.
Figure legends
Fig. 1:Indirect paths between problem-solving, trait anxiety, and
self-efficacy, and ability to function as therapist in emergency situations (MHO self-efficacy).
References
1. Bandura A (1982) Self-efficacy mechanism in human agency. Am Psychologist 37: 122-147.
2. Bandura A (1997) Self-efficacy: The exercise of control. New York: W.H. Freeman and Co.
3. D'Zurilla TJ, Chang EC (1995) The relations between social problem solving and coping. Cognit Ther Res 19: 547-562.
4. Lazarus RS (1993) Coping theory and research: Past, present, and future. Psychosom Med 55: 234-247. [Crossref]
5. Rudd, M. D., Rajab, M. H., & Dahm, P. F. (1994) Problem-solving appraisal in suicide ideators and attempters. Am J Orthopsychiatry 64: 136-149. [Crossref]
6. Lazarus RS, Folkman S (1984) Stress, appraisal and coping. New-York: Springer Publishing Company.
7. Clum GA, Canfield D, Van Arsdel M, Yang B, Febbraro G, et al. (1997) An expanded etiological model for suicide behavior in adolescents: Evidence for its specificity relative to depression. J Psychopathol Behav Assess 19: 207-222.
8. Dixon WA, Heppner PP, Anderson WP (1991) Problem-solving appraisal, stress, hopelessness, and suicide ideation in a college population. J Couns Psychol 38: 51-56.
9. Dixon WA, Heppner PP, Rudd MD (1994) Problem-solving appraisal, hopelessness, and suicide ideation: Evidence for a mediational model. J Couns Psychol 41: 91-98.
10. Albrecht K (2010) Stress and the manager. New York: Simon and Schuster.
11. Southwick SM, Litz BT, Charney D, Friedman MJ (Eds.). (2011) Resilience and mental health: Challenges across the lifespan. Cambridge, UK: Cambridge University Press.
12. Folkman S (2011) Stress, health and coping: An overview. In S. Folkman & P.E. Nathan (Eds.), The Oxford handbook of stress, health, and coping (pp. 3-14). New York: Oxford University Press.
13. Baumeister RF, Leary MR (1995) The need to belong: Desire for interpersonal attachments as a fundamental human motivation. Psychol Bull 117: 497-529. [Crossref]
14. DeWall CN, Baumeister RF (2006) Alone but feeling no pain: Effects of social exclusion on physical pain tolerance and pain threshold, affective forecasting, and interpersonal empathy. J Pers Soc Psychol 91: 1-15. [Crossref]
15. Watson PJ, Ritchie EC, Demer J, Bartone P, Pfefferbaum BJ (2006) improving resilience trajectories following mass violence and disaster. In E.C. Ritchie, P.J. Watson, & M.J. Friedman (Eds.). Interventions following mass violence and disasters: Strategies for mental health practice (pp. 37-53). New York: Guilford Press.
16. Chen G, Gully SM, Eden D (2001) Validation of a new general self-efficacy scale. Organizational Research Methods 4: 62-83.
17. Judge TA, Larsen RJ (2001) Dispositional affect and job satisfaction: A review and theoretical extension. Organ Behav Hum Decis Process 86: 67-98.
18. Baumeister RF, DeWall CN, Ciarocco NJ, Twenge JM (2005) Social exclusion impairs self-regulation. J Pers Soc Psychol 88: 589-604. [Crossref]
19. Dolbier CL, Steinhardt MA (2000) The development and validation of the Sense of Support Scale. Behav Med 25: 169-179. [Crossref]
20. Fernandez ME, Mutran EJ, Reitzs DC (1998) Moderating the effects of stress on depressive symptoms. Res on Aging 20: 163-182.
21. Sarason IG, Levine HM, Basham RB, Sarason BR (1983) Assessing social support: The Social Support Questionnaire. J Pers Soc Psychol 44: 127-139.
22. Stice E, Ragan J, Randall P (2004) Prospective relations between social support and depression: Differential direction of effects for parent and peer support. J Abnorm Psychol 113: 155-159. [Crossref]
23. Orbach I, Blomenson R, Mikulincer M, Gilboa-Schechtman E, Rogolsky M, et al. (2007) Perceiving a problem-solving task as a threat and suicidal behavior in adolescents. J Soc Clin Psychol 26: 1010-1034.
24. Gaudry E, Vagg P, Spielberger CD (1975) Validation of the state-trait distinction in anxiety research. Multivariate Behav Res 10: 331-341. [Crossref]
25. Benedek DM, Fullerton C, Ursano RJ (2007) First responders: Mental health consequences of natural and human-made disasters for public health and public safety workers. Annu Rev Public Health. 28: 55-68. [Crossref]
26. Van Der Veer G, Francis FT (2011) Field-based training for mental health workers, community workers, psychosocial workers and counsellors: A participant-oriented approach. International J of Mental Health, Psychosocial Work & Counseling in Areas of Armed Conflict 9: 145-153.
27. Zakour MJ (1996) Geographic and social distance during emergencies: A path model of interorganizational links. Soc Work Res 20: 19-29.
28. Raphael B, Singh B, Bradbury L, Lambert F (1983) Who helps the helpers? The effects of disaster on rescue workers. OMEGA-Journal of Death and Dying 14: 9-20.
29. Young BH, Ruzek JI, Wong M, Salzer MS, Naturale AJ (2006) Disaster mental health training: Guidelines, considerations, and recommendations. In E.C. Ritchie, P.J. Watson, & M.J. Friedman (Eds.). Interventions following mass violence and disasters: Strategies for mental health practice (pp. 54-79). New York: Guilford Press.
30. McCarroll JE (2005) Disaster psychiatry: Intervening when nightmares come true. J Nerv Ment Dis 193: 701-702.
31. Haans T (2006) Intervention. International Journal of Mental Health, Psychosocial Work & Counseling in Areas of Armed Conflict 4: 95-96.
32. Rogge ME (2003) The future is now: Social work, disaster management, and traumatic stress in the 21st century. J Soc Serv Res 30: 1-6.
33. Voelker R (2006) Post-Katrina mental health needs prompt group to compile disaster medicine guide. JAMA, 295: 259-260.
34. West C, Bernard B, Mueller C, Kitt M, Driscoll R, et al. (2008) Mental health outcomes in police personnel after Hurricane Katrina. J Occup Environ Med 50: 689-695. [Crossref]
35. Zhang F, Xin Y, Chen D, Chen Y (2010) Research of police's mental health and influence factors in badly damaged regions one year after earthquake. Chinese J Clin Psychol 18: 76-78.
36. Yanay U, Benjamin S (2005) The role of social workers in disasters: The Jerusalem experience. International Social Work 48: 263-276.
37. Lurie O (2007) Chisun kognetivi kehachanat hagorem haenoshi lamilchama beyechidot cheil haavir [Cognitive inoculation in preparing the human factor for combat in air force units]. Sihot 21: 182-189.
38. Shelef L, Laur L, Raviv G, Fruchter E (2015) A military suicide prevention program in the Israeli Defense Force: A review of an important military medical procedure. Disaster Mil Med 1: 1-16. [Crossref]
39. Salmon TW (1917) The care and treatment of mental diseases and war neuroses ("shell shock") in the British Army. New York: War Work Committee of the National Committee for Mental Hygiene, Inc.
40. Brown LM, Beutler LE, Breckenridge JN, Zimbardo PG (2007) Psychology of terrorism. New York: Oxford University Press.
41. Busuttil W, Busuttil A (1997) Debriefing and crisis intervention. In D Black, M Newman, J Harris-Hendriks, & G Mezey (Eds.), Psychological trauma: A developmental approach (pp. 238–249). London: Gaskell.
42. Adler AB, Bliese PD, McGurk D, Hoge CW, Castro CA (2011) Battlemind debriefing and battlemind training as early interventions with soldiers returning from Iraq. Sport Exerc Perform Psychol 1: 66-83.
43. Bisson JI (2003) Single-session early psychological interventions following traumatic events. Clin Psychol Rev 23: 481-499. [Crossref]
44. Forneris CA, Gartlehner G, Brownley KA, Gaynes BN, Sonis J (2013) Interventions to prevent post-traumatic stress disorder: A systematic review. Am J Prev Med 44: 635-650. [Crossref]
45. Hawker DM, Durkin J, Hawker DS (2011) To debrief or not to debrief our heroes: That is the question. Clin Psychol Psychother 18: 453-463. [Crossref]
46. Quarantelli EL (2006) Catastrophes are different from disasters: Some implications for crisis planning and managing drawn from Katrina, Understanding Katrina: Perspectives from the social sciences.
47. Bar-Tal Y, Lurie O, Glick D (1994) The effect of gender on the stress process of Israeli soldiers during the Gulf War. Anxiety Stress Coping 7: 263-276.
48. Solomon Z, Gelkopf M, Bleich A (2005) Is terror gender-blind? Gender differences in reaction to terror events. Soc Psychiatry Psychiatr Epidemiol 40: 947-954. [Crossref]
49. Israel Security Agency (n.d). Operation pillar of defense.
50. Schwarzer R, Jerusalem M (1995) Generalized Self-Efficacy Scale. In J. Weinman, S. Wright, & M. Johnston (Eds.). Measures in health psychology: A user’s portfolio. Causal and control beliefs (pp. 35-37). Windsor, UK: NFER-NELSON.
51. Muthén LK, Muthén BO (1998-2010). Mplus user’s guide (sixth ed.). Los Angeles, CA: Muthén & Muthén.
52. Spielberger CD, Gorsuch RL, Lushene R, Vagg PR, Jacobs GA (1983) Manual for the State-Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press.
53. Hayes AF (2009) Beyond Baron and Kenny: Statistical mediation analysis in the new millennium. Commun Monogr 76: 408-420