Application of Tenodesis for an Extremely Rare Hand Extensor Injury in an Athlete: A Case Report
A B S T R A C T
Spontaneous tendon ruptures of the wrist are a rare pathology, usually secondary to rheumatoid arthritis or distal radius fractures and most commonly evolving the extensor pollicis longus. Sport-related etiology is a growing tendency of this pathology. As far as the authors know, this is one of the first sport-related extensor carpi radialis brevis (ECRB) isolated spontaneous rupture described in the literature. We describe a case of a 41 year-old female amateur kickboxer who developed acute dorsal radial pain in the right wrist during practice. After attempting conservative treatment for 4 months with rest and NSAIDs she recurred at our clinic. Local pain at dorsal wrist extension was observed. MRI demonstrated an isolated ECRB rupture with associated fibrous tissue proximal to the extensor retinaculum. Surgical management was proposed and consisted of fibrous tissue debridement and ECRB-ECRL tenodesis. At 3 months of follow-up the patient reported return-to-play with impaired wrist motion and mild pain at maximum wrist extension. At 12 months of follow-up the patient was completely recovered and asymptomatic. Isolated tendon ruptures are a rare pathology, causing extreme pain and disability in the sport setting. Surgical management of this ECRB tendon rupture by tenodesis allowed for appropriate pain control and functional results and early return-to-play.
Keywords
Sports medicine, hand extensor injuries, tenodesis
Introduction
Hand extensor tendon traumatic injuries are common lesions specially among young athletes [1]. Several risk factors may lead to this type of injuries such as professional exposure to repetitive hand movements, medications such as fluoroquinolones, corticosteroid use and also pathologies such as rheumatoid arthritis. Furthermore, anatomical variations such as a carpal boss may be the cause of these injuries [2-5]. When in the context of sport injuries, these are frequently associated with striking sports such as boxing or kickboxing. In these sports, due to the emphasis on punching movements against hard targets with a closed fist, the hand is subject to extremely high levels of axial force, which, especially when associated with poor technique/amateur practice, may lead to extensor tendon injuries [6].
Insertional injuries of ECRB/ECRL tendons are usually due to forced hyperflexion in an actively extended wrist [7]. Avulsion injuries of these tendons, in the base of the metacarpals are rare, due to strong capsule/ligament attachments [8]. The few cases described in the literature mostly involve young adults practicing high energy sport activities or falls [9].Clinical diagnosis is not always simple, as ecchymosis may not be present in the acute setting and the patient may present only with non-specific dorsal wrist pain and difficulty in dorsiflexion [8, 10]. X rays and CT- scans often do not diagnose this type of pathology even when a bony avulsion is present [7].
When midsubstance tears are present, diagnosis can best be performed using MRI studies. As such, these lesions can be easily missed. Midsubstance extensor tendon tears are extremely rare and usually secondary to tendon atrophy and subsequent tear often due to attritional damage as is the case in rheumatoid or post-traumatic deformities [2, 3, 11]. Treatment usually comprises conservative measures with surgical treatment being recommended for the treatment of the insulting factor, as for the treatment of attritional rupture do to dorsal carpal boss [12, 13]. In this case report we describe the successful application of a tenodesis technique in the treatment of a sports related ECRB midsubstance rupture.
Case Description
A 41-year-old female, with no relevant past medical history came to our clinic due to sudden radial sided pain in the dorsal wrist. She described the onset of pain after a kickboxing training session, which she practiced twice a week in an amateur regime. The pain was located in the base of the dorsal aspect of the 2nd /3rd metacarpals and was associated with impaired wrist motion, mainly extension, which compromised her daily routine activities. At first, she tried to manage the case with rest and NSAID medication, with non-satisfactory results. Upon physical examination, there was noted radial dorsal side pain associated with wrist extension strength deficit when comparing with the contralateral side. MRI exam demonstrated an isolated distal ECRB rupture with associated fibrous tissue being present proximal to the extensor retinaculum (Figure 1). Surgical management of this lesion was decided.
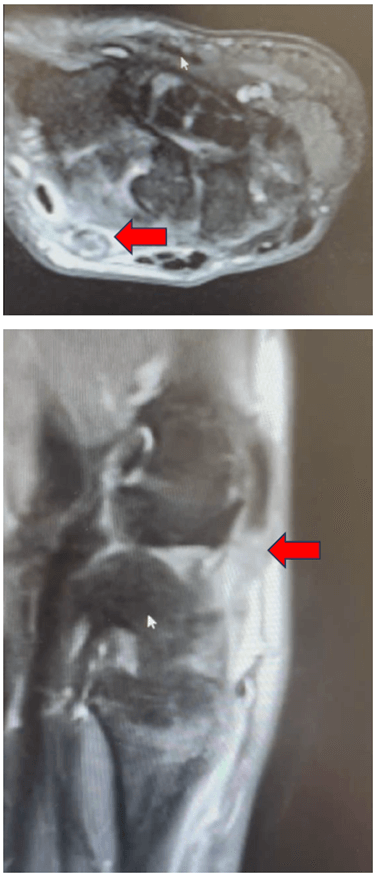
Figure 1: MRI studies showing lesion of the ECRB tendon (arrow).
Surgical Technique
Under a brachial plexus block, a straight skin incision was made over the dorsum of his left wrist, lining with the Lister´s tubercle (Figure 2). Careful dissection was performed, incising and opening the extensor retinaculum. ECRB distal midstubstance rupture was then evident with the distal limb of the tendon being attached to the proximal limb by a slim fibrous tissue connection (Figure 3). Degenerative fibrous tissue was carefully debrided of the ECRB. The remaining healthy proximal and distal limbs of ECRB were subjected to tenodesis with ECRL, by a side-by-side technique, using P.D.S. suture (Figure 4). Judicious closure and dressing were applied, and a wrist extension cast was used.
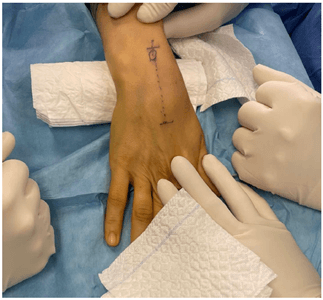
Figure 2: Surgical approach.
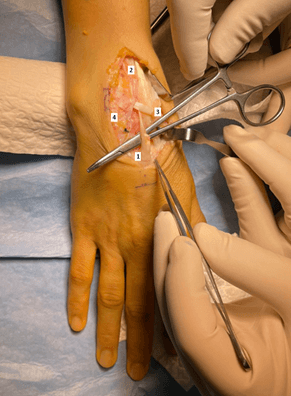
Figure 3: ECRB Rupture. 1) ECRB; 2) ECRL; 3) EPL; 4) Extensor retinaculum.
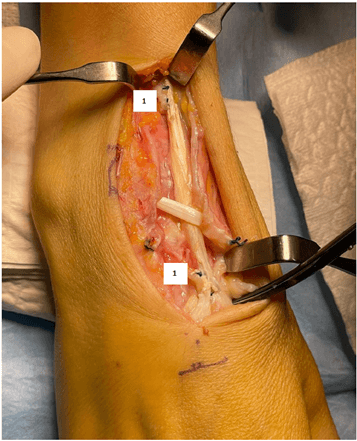
Figure 4: ECRB-ECRL tenodesis. 1) Side-to-side suture.
Results
Arm suspension and wrist cast immobilization were used for a month after surgery. After removing the cast, light ROM exercises were permitted, and physical therapy was commenced. At 3 months of follow-up, the patient reported decreased pain and gradual return to normal daily activities. At 12 months of follow-up, the patient reported only residual pain (maximum with daily activities of VAS 2), no activity restrains and identical ROM when comparing to the contralateral side.
Discussion
To our knowledge this case report represents the first published case of a sports trauma ECRB midsubstance tear. Accounts of isolated ECRB tears are rare, and mostly associated with bony avulsion, most of them treated with osteosynthesis of the avulsion fractures of the base of the 3rd metacarpal bone [8, 9, 14]. ECRB lesions may be important to overall wrist function due to the importance of this muscle in wrist dorsiflexion, and conservative and surgical treatment are both valid options [15]. Huffaker et al., described an isolated ECRB midsubstance tear secondary to a dorsal scaphoid osteophyte, which was treated conservatively [2]. Gurich et al. reported good clinical results using ECRB-ECRL tenodesis in a late- presentation bony avulsion injury of both tendons [10].
As in this case, clinical signs were non-specific and MRI study was instrumental to the diagnosis of this pathology. There are several techniques described for the treatment of acute setting ECRB avulsion injury [9]. These all depend on a bony fragment to allow for osteosynthesis. When a midsubstance tear is present, treatment can either be conservative or surgical using side-to-side tenodesis with ECRL [2, 10]. In our case, surgical treatment was chosen as conservative treatment did not prove to resolve the patients functional and pain symptoms. ECRB-ECRL tenodesis and inflammatory tissue debridement allowed for local pain resolution as well as patient functional improvement.
This is, as far as the authors are aware, the first report of isolated insertional midsubstance tear of ECRB in the sport setting. Treatment with side-to-side ECRB-ECRL tenodesis allowed for a quick return-to-work and good patient satisfaction.
Abbreviations
ECRB: Extensor Carpi Radialis Brevis
NSAIDs: Non-Steroid Anti-Inflammatory Drugs
MRI: Magnetic Resonance Imaging
ECRL: Extensor Carpi Radialis Longus
Article Info
Article Type
Case ReportPublication history
Received: Thu 22, Feb 2024Accepted: Fri 12, Apr 2024
Published: Fri 26, Apr 2024
Copyright
© 2023 João Pereira. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.IJSCR.2024.01.03
Figures & Tables
References
1.
Dy CJ, Rosenblatt L, Lee SK (2013) Current methods and
biomechanics of extensor tendon repairs. Hand
Clin 29: 261-268. [Crossref]
2.
Huffaker SJ, Christoforou DC, Jupiter JB (2012) Spontaneous
rupture of the extensor carpi radialis brevis in a 51-year-old man: case
report. J Hand Surg Am 37: 1221-1224.
[Crossref]
3.
Williamson SC, Feldon P (1995) Extensor tendon ruptures in
rheumatoid arthritis. Hand Clin. Aug
11: 449-459. [Crossref]
4.
Hussen NHA, Qadir SH, Rahman HS, Hamalaw YY, Kareem PSS, et
al. Long-term toxicity of fluoroquinolones: a comprehensive review. Drug Chem Toxicol 28: 1-12. [Crossref]
5.
Szarfman A, Chen M, Blum MD (1995) More on fluoroquinolone
antibiotics and tendon rupture. N Engl J
Med 332: 193. [Crossref]
6.
Loosemore M, Lightfoot J, Gatt I, Hayton M, Beardsley C
(2017) Hand and Wrist Injuries in Elite Boxing: A Longitudinal Prospective
Study (2005-2012) of the Great Britain Olympic Boxing Squad. Hand (N Y) 12: 181-187. [Crossref]
7.
Robert N, Zbili D, Bellity J, Doursounian L, Mauprivez R
(2014) Avulsion fracture of the extensor carpi radialis longus carpal insertion
due to a basketball injury: case report and literature review. Chir Main 33: 410-412. [Crossref]
8.
Johnson AE, Puttler EG (2006) Avulsion of the extensor carpi
radialis brevis insertion: a case report and review of the literature. Mil Med 171: 136-138. [Crossref]
9.
Turker T, Capdarest Arest N (2013) Open isolated extensor
carpi radialis brevis avulsion injury: a case report. Hand (N Y) 8: 354-357. [Crossref]
10. Gurich
Jr. RW, Tanksley Jr. JA, Pappas ND
(2013) Late repair of combined extensor carpi radialis longus and brevis
avulsion fractures. Orthopedics 36:
766-769. [Crossref]
11. Vaughan
Jackson OJ. Rupture of extensor tendons by attrition at the inferior radio-
ulnar joint; report of two cases. J Bone
Joint Surg Br 30B: 528-530. [Crossref]
12. Park
MJ, Namdari S, Weiss AP (2008) The carpal boss: review of diagnosis and
treatment. J Hand Surg Am 33:
446-449. [Crossref]
13. Clarke
AM, Wheen DJ, Visvanathan S, Herbert TJ, Conolly WB (1999) The symptomatic
carpal boss. Is simple excision enough? J
Hand Surg Br 24: 591-595. [Crossref]
14. Breeze SW, Ouellette T, Mays MM (2009) Isolated avulsion fracture of the extensor carpi radialis brevis insertion due to a boxer's injury. Orthopedics 32: 210. [Crossref]
15. Brand PW, Beach RB, Thompson DE (1981) Relative tension and potential excursion of muscles in the forearm and hand. J Hand Surg Am 6: 209-219. [Crossref]