An Overview of Definition and Approaches to Petroclival Meningioma
A B S T R A C T
Meningiomas account for 20 to 25% of all intracranial tumors and 10% are seen in the posterior fossa. Petroclival tumors are defined as arising from the upper two thirds of the clivus, medial to the trigeminal nerve at the petroclival junction. Brain CT scan and MRI are routinely used to evaluate tumor anatomy. The petrous temporal bone is a hindrance to resection of these tumors. Oftentimes neurosurgeons are unskilled with the anatomy of the petrous bone, and so suboccipital and pterional routes are usually preferred. Some authors have encouraged using traditional neurosurgical approaches to these tumors. In this manuscript we review tumor location and approaches used for resection of these challenging tumors.
Keywords
Meningioma, petroclival, approaches
Introduction
Meningiomas account for 20 to 25% of all intracranial tumors and 10% are seen in the posterior fossa. Of posterior fossa meningiomas, those rising from the petroclival region account for 5 to 11% of meningiomas and thus 0.15% of all intracranial tumors. Male to female ration is 1 to 4. Petroclival tumors are defined as arising from the upper two thirds of the clivus, medial to the trigeminal nerve at the petroclival junction, often extent to the middle and approaches posterior cranial fossae and can involve the posterior cavernous sinus through the Meckel cave [1]. Growth rates were 0.81 mm/yr (Diameter) and 0.81 cm3/yr (Volume). When only growing tumors were measured, the mean growth rates were 1.16 mm/yr (Diameter) and 1.10 cm3/yr (Volume). Untreated tumors may grow at a dissimilar rate than resected tumors [2]. The petrous temporal bone is a hindrance for tumor resection in this location. Oftentimes neurosurgeons are unskilled with the anatomy of the petrous bone, and so suboccipital and pterional routes are preferred. Some authors have encouraged using traditional neurosurgical approaches to these tumors.
Discussion
To select an appropriate approach all patients typically undergo CT to examine the bony architecture and relationships between the skull base and tumor. MRI is routinely used to evaluate presence of edema in the brainstem and soft-tissue relationships between the CNS and the tumor. Angiography to evaluate the arterial supply and relationship to major vessels is sometimes useful. Selection of approach depends on location, size, extension of the tumor, venous sinus anatomy and preoperative hearing evaluation.
Strategies to Overcome the Petrous Temporal Bone as an Obstacle
Resection of the petrous apex with the middle fossa approach. Resection of presigmoid, retrolabyrinthine petrous bone with the posterior petrosal approach. Resection of the entire petrous bone with complete petrosectomy. Mayberg and Symon believed that the combined subtemporal-posterior fossa approach provided the best results, as did Guthrie et al. Various alterations of this approach have been described by Samii et al. and Hakuba et al. Al-Mefty and co-workers have described in detail a petrosal approach for these tumors [3].
Tumors that are medial to the internal auditory canal and extent to both middle and posterior cranial fossae are often best treated with a combined transpetrosal approach, which is particularly true if there is a preoperative hearing deficit. The anterior petrosal approach is best appropriate for smaller petroclival meningiomas that do not spread lateral to the IAM. Once a tumor has extended farther into the posterior fossa, lateral to the IAM, a posterior petrosal approach should be used. A retrosigmoid craniotomy remains a workhorse surgical approach for most petroclival tumors of any size (Figure 1). More Recently, the Endoscopic Endonasal Approach has been "expanded" to the petroclival region. This approach should be favored for extradural midline tumors (chordomas, chondrosarcomas) or for cystic lesions when drainage is crucial [4].
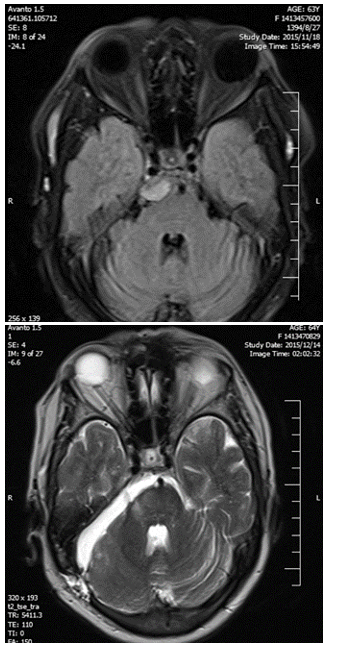
Figure 1: Pre- and post-operative MRI of small right petroclival meningioma resected by retrosigmoid approach.
GTR is only reported in an average of 49% of patients. Many high-volume surgical centers have abandoned GTR for NTR or STR later in their practice. Most describe that STR/NTR does not have an increased risk or recurrence compared with GTR in most series [5]. Attempts at accomplishing gross- or near-total resections are associated with an increased rate of morbidity and mortality. (Adjunctive treatment options such as stereotactic radiosurgery is attractive options). There has been a tendency to accept subtotal resections in an effort to minimize neurological morbidity [6]. Radiation therapy is used if a satisfactory decompression cannot be implemented or there is regrowth after radical subtotal removal [3].
Motor deficits and facial nerve morbidity are the common postoperative neurological complications. CSF leaks occur in 10% of patients. In spite of the high morbidity, >75% of patients return to independence at 1 year, many of which will start again employment [5].
Conclusion
Petroclival tumors also infrequent still remain a surgical challenge. The petrous temporal bone is an obstacle for tumor resection in this location. Oftentimes neurosurgeons are unfamiliar with the anatomy of the petrous bone, and so suboccipital and pterional routes are used. Some authors have advocated using traditional neurosurgical approaches to these tumors. The infrequency of the tumor, different treatment philosophies, and variations in reporting, complicate the outcome analysis and so choosing a definite approach for these tumors.
Conflicts of Interest
None.
Abbreviations
IAM: Internal Auditory Meatus
GTR: Gross Total Resection
NTR: Near Total Resection
STR: Subtotal Resection
Article Info
Article Type
Review ArticlePublication history
Received: Mon 05, Oct 2020Accepted: Sat 07, Nov 2020
Published: Mon 24, May 2021
Copyright
© 2023 Alireza Khoshnevisan. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.AJOS.2020.01.01
Figures & Tables
References
1.
Richard Winn H
(2017) Youmans & Winn neurological surgery. 7th Edition, Elsevier
Philadelphia 1108.
2.
Fountain DM, Soon
WC, Matys T, Guilfoyle MR, Kirollos R et al. (2017) Volumetric growth rates of
meningioma and its correlation with histological diagnosis and clinical
outcome: a systematic review. Acta Neurochir (Wien)159: 435-445.
[Crossref]
3.
Ojemann Robert G
(1992) Convexity Meningiomas. Clin Neurosurg 40: 321-383.
4.
Jacquesson T,
Berhouma M, Tringali S, Simon E, Jouanneau E (2015) Which routes for
petroclival tumors? A comparison between the anterior expanded endoscopic
endonasal approach and lateral or posterior routes. World Neurosurg 83:
929-936. [Crossref]
5.
DiLuna ML,
Bulsara KR (2010) Surgery for Petroclival Meningiomas: A Comprehensive Review
of Outcomes in the Skull Base Surgery Era. Skull Base 20: 337-342. [Crossref]
6.
Xu F, Karampelas
I, Megerian CA, Selman WR, Bambakidis NC (2013) Petroclival meningiomas: an
update on surgical approaches,decision making, and treatment results. Neurosurg
Focus 35: E11. [Crossref]