Adolescent High-Risk Behaviors and Orofacial Trauma
A B S T R A C T
Aim: The objective of the study was to investigate if there was a relationship between high risk behaviors among adolescents and orofacial trauma.
Material and Methods: The study used a cross-sectional retrospective design with data collected from electronic health records of over 4,000 patients treated in the Department of Pediatric Dentistry at the University of Pittsburgh School of Dental Medicine from May 2009 through September 2013. This study was approved by the University of Pittsburgh Institutional Review Board. Risk factors for trauma were obtained from each patient’s medical and social history and included tobacco, alcohol and illicit drug use, tattoos, piercings, and mouthguard use during sports. Outcome measures used were history of broken bones or orofacial trauma. The odds ratios (OR) and 95% confidence intervals (CI) of each risk factor in increasing risk for trauma outcomes were calculated. Chi-square tests were also performed with an alpha of 0.05.
Results and Conclusions: A total of 2,609 patients were included in this study. Males (N=1,340) had statistically more often orofacial trauma than females, and were statistically more often exposed to all risk factors (tobacco, alcohol and illicit drug use, tattoos, and physical altercations) than females with the exception of using piercings in body parts other than the ears and not wearing mouthguard for sports. Wearing mouthguard for sports decreased in 50% the risk of orofacial trauma (OR=0.53; 95% CI 0.42-0.68; p=0.00000001). Tobacco use and physical altercations increased the chance of broken bone, fractured tooth, and orofacial trauma in 2-fold (smoking, OR=1.85-2.28, 95% CI 1.3-2.96; physical altercations, OR=1.9-2.34; p=0.0005). Drinking and using illicit drugs increased the risk of broken bone (OR=1.9, 95% CI 1.37- 2.64; p=0.0001). Use of mouthguards for sports dramatically reduced the risk of orofacial trauma. Tobacco, alcohol and illicit drug use, and getting into physical altercations increased the risk of orofacial trauma.
Keywords
Adolescents, dental trauma, smoking, alcohol drinking, mouth guard
Introduction
Orofacial trauma can be defined as pain resulting from forces inflicted on the mouth, jaw, face, and surrounding oral soft tissues. This trauma is considered a public health problem among children and adolescents due to significant prevalence rates, psychosocial effects on quality of life, and high treatment costs [1]. Numerous biological factors predispose one for orofacial trauma, including: the male gender, an increase in overjet, inadequate lip protection, violence, and socio-economic status [2, 3].
Adolescence is a transitional stage of human development between 12 to 18 years of age in which substantial physical and psychological transformations occur [4]. This stage is associated with the onset of puberty, considerable physical growth, brain maturation, hormonal changes, and heightened risk taking. The manifestation of behaviors such as fighting, substance abuse, sexual intercourse, rebelliousness, and tests of invincibility affects not only academic performance, relationships, and health – but specifically the incidence of orofacial trauma, as well [5].
A modest amount of research has been conducted in different countries with regards to orofacial trauma and a number of different factors such as, socioeconomic status, risk behaviors, and environmental circumstances, have been found to be associated with its occurrence [6, 7]. A considerable number of studies have also suggested the use of mouthguards to reduce the severity of sports-related injuries to the teeth and soft tissues. Historically, mouthguard usage has been encouraged or required to reduce concussions and dental injuries [8]. This thought has contributed to increased implementation of educational programs in school classrooms and athletic departments [9]. However, there is still the need for more evidence and clarified understanding of the risk factors, which will allow that preventive measures be amplified.
As a dentist, it is essential to understand the physiological and physical changes that occur during adolescence to better treat patients in that age group. With better understanding of the causes and effects behind the occurrence of these changes, dentists can have a greater grasp on why adolescents are associated with high risk behaviors. This allows dentists to provide their adolescent patients with more comprehensive planning, decision-making, and intervention in the provision of their care [10]. High-risk behaviors include tobacco, alcohol, illicit drug use, tattoos, piercings, and no mouthguard use during sports. The Centers for Disease Control and Prevention (CDC) states that high-risk behaviors contribute greatly to leading causes of death, disability, and social problems among youth in the United States. The aim of this study was to investigate the association between high risk behaviors and orofacial trauma among adolescent patients.
Material and Methods
This study consisted of a cross-sectional retrospective design using data collected from the electronic health records of patients treated in the Department of Pediatric Dentistry at the University of Pittsburgh School of Dental Medicine from May 2009 through September 2012. These health records are housed via the Axium software. Each health record was extrapolated from the software format into a Windows Excel spreadsheet. The protocol of this study was approved by the University of Pittsburgh Institutional Review Board (IRB # PRO09030552). A total of 2,609 patient records were included in this study. The odds ratios (OR) and 95% confidence intervals (CI) of each risk factor for trauma outcomes were calculated. Chi square tests were performed with an alpha of 0.05.
The following questions were asked to the guardian and patient as both were present while the information was collected:
Does your child use tobacco products?
Does your child use alcohol or street drugs?
Do you have any forms of body piercings?
Have you ever been in a physical altercation?
Have you ever broken any bones?
Have you ever had trauma to your face or head?
Do you use an athletic mouthguard when playing contact sports?
Answers were provided by the patient’s guardian in a “yes” or “no” format, with the opportunity to elaborate on “yes” answers. Patients under the age of 12 were not included in the analysis of trauma to the permanent dentition. Answers insinuating avulsed teeth were included in results for orofacial trauma. The population was analyzed based on biological sex (male and female) and age ranges (12-14 years old, 15-16 years old, and 17-18 years old). These ranges were used based on likely participation in activities such as driving in ages 15-16.
Results
Males (N=1,340) were twice more likely than females (N=1,269) to have orofacial trauma (OR=2.07, 95% C.I. 165-2.59, p=0.00000001), and were three times more likely to be exposed to risk factors (tobacco, alcohol, and illicit drug use, tattoos, and physical altercations) than females (OR=2.98, 95% C.I. 2.37-3.74, p=0.00000001), with the exception of piercings in body parts other than ears (OR=1.34, 95% C.I. 0.97-1.86, p=0.00000001), and the risk factor of not wearing a mouthguard during sports (OR=6.43, 95% C.I. 5.07-8.15, p=0.000000001) (Figure 1).

Figure 1: Frequency of risk factors among males and females.
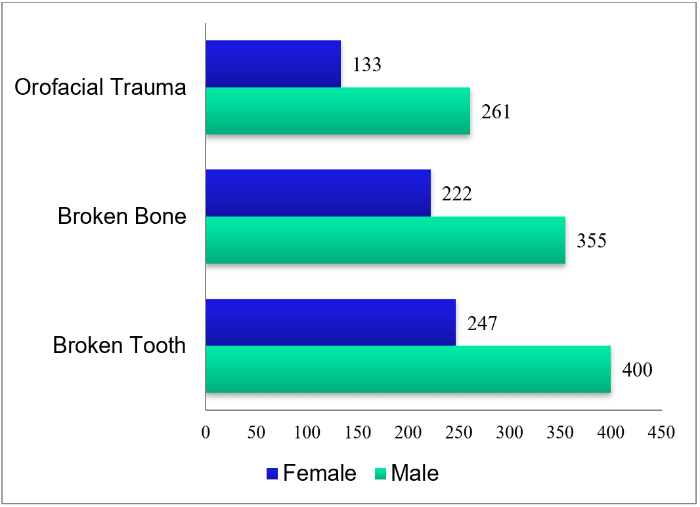
Figure 2: Frequency of trauma between males and females.
Wearing a mouth guard for sports decreased in 50% of the risk for orofacial trauma (OR=0.53; 95% CI 0.42-0.68; p=0.00000001). Tobacco use and physical altercations increased the risk of broken bone, avulsed and/or fractured teeth, and orofacial trauma by 2-fold (smoking OR=1.85-2.28, 95% CI 1.3-2.96; physical altercations OR=1.9-2.34, 95% CI 1.37-2.64; p=0.0005). Alcohol and illicit drug use increased the risk of broken bones (OR=1.9, 95% CI 1.37-2.64; 0.0001) (Figure 2).
Discussion
It is essential for dentists who treat adolescent patients to understand the physiological and psychological changes that occur during adolescent development. The prevalence of traumatic dental injuries is as high as one fourth of all school children and nearly one third of all adults [11]. The dentist is responsible for understanding how and why these changes may contribute an increased likelihood of oral trauma in order to provide the patient with comprehensive and preventative care. High-risk behaviors may have a direct or indirect association with trauma that the dentist should be willing to address as concerns to the patient and/or guardian.
The use of mouthguards during sports in adolescence statistically protects against the risk of orofacial trauma. It is important to question patients and guardians about participation in activities that may benefit from the use of a mouthguard. While the correlation between orofacial trauma and type of mouthguard was not determined, dentists have the opportunity to provide a well-fitting custom-made mouthguard which is more comfortable, and therefore easier for patients to comply with wearing [12].
Tobacco, alcohol, illicit drug use, and physical altercations all increase the risk of orofacial trauma. While these behaviors may be detrimental to adolescents in their own direct ways, a relationship to the oral cavity may not be as obvious with tobacco, alcohol, or drug use. If there is any suspicion of patients’ participation in these activities, it is important to address the risks associated with oral health, which may not be as obvious to the patient or guardian. In a similar situation, tobacco use and physical altercations increase the risk of broken bones. While tobacco use, in terms of oral cancer risks, may be more commonly known, an association with broken bones is likely less obvious. This correlation can be related to any number of compounding factors that are also associated with tobacco use. For example, tobacco use may also relate to use of alcohol and increase the likelihood for participating in risky behaviors.
Being involved in physical altercations, however, is more obviously a direct cause of trauma that can be avoided. Boys, in particular, are known to be involved in more physical games and indulge in more violent behaviors [13]. Participation in one behavior may also open the opportunity to become involved in additional risky behaviors. Prevention can be attended to by acknowledging the risks of current behaviors. A multi-factorial relationship exists between high risk behaviors and orofacial trauma [14]. This correlation can be influenced by a number of compounding factors, for example, adolescents who are participating in physical altercations. These patients may need more emotional support included with their treatment plan. Prevention of further trauma requires the dentist to address these issues with the patient and guardian.
Answers collected in regards to patients’ activities were answered by the guardian, or in the presence of a guardian. Willingness to answer truthfully to participating in high risk behaviors may be diminished in these patients given the circumstances. Patients may be fearful of being repented by their parents or guardians for admitting to activities such as smoking tobacco or using alcohol and drugs. Therefore, a stronger correlation may exist than was represented by the answers from this study.
Conflicts of interest
The authors have no conflict of interest to declare.
Acknowledgements
The authors thank all participants and their families.
Data Availability
All data reported here is available upon request.
Funding
This study was funded by discretionary funds of the Department of Pediatric Dentistry, University of Pittsburgh School of Dental Medicine.
Article Info
Article Type
Research ArticlePublication history
Received: Mon 08, Jul 2019Accepted: Tue 13, Aug 2019
Published: Fri 20, Sep 2019
Copyright
© 2023 Adriana Modesto. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.ORD.2019.01.01
Figures & Tables
References
- Baig Enver M, Marcenes W, Stansfeld SA, Bernabé E et al. (2016) Alcohol Consumption at Age 11-12 Years and Traumatic Dental Injuries at Age 15-16 Years in School Children from East London. Dent Traumatol 32: 361-366. [Crossref]
- Filho PM, Jorge KO, Paiva PC, Ferreira EF, Ramos-Jorge ML et al. (2014) The Prevalence of Dental Trauma and Its Association with Illicit Drug Use among Adolescents. Dent Traumatol 30: 122-127. [Crossref]
- Goulart DR, Durante L, de Moraes M, Asprino L (2015) Characteristics of Maxillofacial Trauma Among Alcohol and Drug Users. J Craniofac Surg 26: 783-786. [Crossref]
- Paiva PC, Paiva HN, Oliveira Filho PM, Lamounier JA, Ferreira RC et al. (2015) Prevalence of Traumatic Dental Injuries and Its Association with Binge Drinking among 12-year-olds: A Population-based Study. Int J Pediatr Dent 25: 239-247. [Crossref]
- Jorge KO, Oliveira Filho PM, Ferreira EF, Oliveira AC, Vale MP et al. (2012) Prevalence and Association of Dental Injuries with Socioeconomic Conditions and Alcohol/drug Use in Adolescents between 15 and 19 Years of Age. Dent Traumatol 28: 136-141. [Crossref]
- Oliveira Filho PM, Jorge KO, Ferreira EF, Ramos-Jorge ML, Tataounoff J et al. (2013) Association between Dental Trauma and Alcohol Use among Adolescents. Dental Traumatol 29: 372-377. [Crossref]
- Ramos-Jorge ML, Peres MA, Traebert J, Ghisi CZ, de Paiva SM et al. (2008) Incidence of Dental Trauma among Adolescents: A Prospective Cohort Study. Dent Traumatol 24: 159-163. [Crossref]
- Glenn Beachy (2004) Dental Injuries in Intermediate and High School Athletes: A 15-Year Study at Punahou School. J Athl Train 39: 310-315. [Crossref]
- de Paiva HN, Paiva PC, de Paula Silva CJ, Lamounier JA, Ferreira E Ferreira E et al. (2015) Is There an Association between Traumatic Dental Injury and Social Capital, Binge Drinking and Socioeconomic Indicators among Schoolchildren? PLoS One 10: e0118484. [Crossref]
- Azami-Aghdash S, Ebadifard Azar F, Pournaghi Azar F, Rezapour A, Moradi-Joo M et al. (2015) Prevalence, etiology, and types of dental trauma in children and adolescents: systematic review and meta-analysis. Med J Islam Repub Iran 29: 234. [Crossref]
- Glendor U (2008) Epidemiology of traumatic dental injuries--a 12 year review of the literature. Dent Traumatol 24: 603-611. [Crossref]
- Tuna EB, Ozel E (2014) Factors Affecting Sports-Related Orofacial Injuries and the Importance of Mouthguards. Sports Med 44: 777-783. [Crossref]
- Vanka A, Ravi KS, Roshan NM, Shashikiran ND (2010) Analysis of Reporting Pattern in Children Aged 7 to 14 Years with Traumatic Injuries to Permanent Teeth. Int J Clin Pediatr Dent 3: 15-19. [Crossref]
- Glendor U (2009) Aetiology and risk factors related to traumatic dental injuries- a review of the literature. Dent Traumatol 25: 19-31. [Crossref]