Journals
A rare case of hiperandrogenism due to oncocytic adrenocortical neoplasm
A B S T R A C T
Oncocytic adrenocortical neoplasm are very rare, with only 150 cases described in the medical literature. Usually, they are diagnosed incidentally on imaging performed for other indications because only approximately 17% are functional masses. Treatment is generally adrenalectomy and laparoscopy can be performed when there is no evidence of malignancy. We report a rare case of a functional oncocytic adrenocortical neoplasm secreting an excess of androgens.
Keywords
Adrenocortical neoplasm, oncocytic neoplasm, hyperandrogenism
Introduction
Oncocytic neoplasms are formed by cells whose characteristic is their eosinophilic and granular cytoplasm caused by the accumulation of mitochondria [1]. They are extremely rare in the adrenal gland. Only 150 cases have been described in the medical literature [2, 3]. Here we are reporting a rare case of a functional oncocytic adrenocortical androgen-secreting neoplasm.
Material and Methods
Patient is a 38-year-old female suffering obesity and hirsutism for many years. She consulted because she had amenorrhea for one year. No history of hypertension or Cushing’s syndrome. After ruling out a gynaecological cause, a computed tomography (CT) was performed and it showed a large mass [98x109x100 mm] in the right adrenal gland, heterogeneous, well circumscribed, with no microcalcifications. Magnetic resonance imaging (MRI) also displayed an 11cm diameter tumour. Other findings in MRI were cholelithiasis and a hepatic haemangioma. Biochemical workup showed high levels of dehydroepiandrosterone (DHEA) [above 1000mcg/dl] together with high levels of testosterone [1.7ng/ml]. There were no increased levels of cortisol, catecholamines, metanephrines, aldosterone, LH, FSH, prolactin, estradiol, progesterone nor tumour markers. A right adrenalectomy and a cholecystectomy were performed through open surgery on account of the size of the lesion as well as suspicion of malignancy. Surgical time was 180 minutes. A seroma was the only complication, which was dealt conservatively. Histological findings revealed an adrenal oncocytic neoplasm with uncertain malignant potential. Macroscopically the tumour measured 13 cm and weighed 580 mg. It had a mitotic index of 1 mitosis x 10 high magnification fields. No atypical mitoses nor venous invasion was detected. Margins of resection were free of tumour. Inmunohistochemistry showed the tumour cells to be positive for melan A and vimentine and negative for p53 and AE1/3. It had a Ki of less than 1%. We decided together with the oncologists that no adjuvant treatment was needed. A clinical control with hormonal tests was scheduled after 4 months. Six months after surgery, the patient is asymptomatic, and she has regained menstruation with regular cycles. Serum chemistries are normal and CT control showed neither local or distant recurrence.
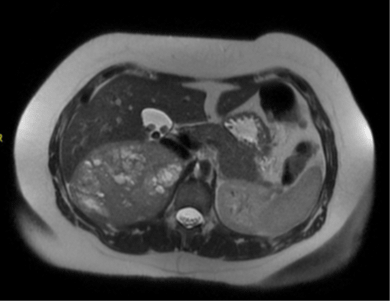
Figure 1: MRI: Mass in right adrenal gland 11cm in diameter, solid, with cystic areas inside but without calcifications, bleeding or macroscopic or intracellular fat.
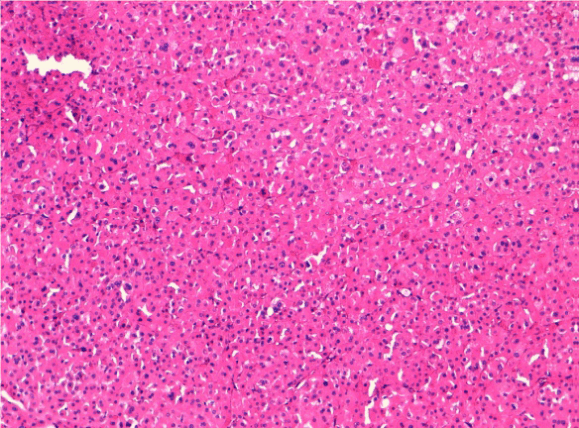
Figure 2: Oncocytic cells with round central nucleus and ample polygonal cytoplasm of eosinophilic and granular type.
Discussions
Oncocytic adrenocortical neoplasms are more frequent in females in their fourth decade [1, 4]. Most of them are diagnosed as incidental findings on CT or MRI and only 17% are functional [5]. There are no typical findings in the imaging tests for these tumours, but heterogeneous appearance, absence of fat, or lack of signal intensity loss in the of MRI’s opposite phase, is a hint in the possible diagnosis [3]. The prognosis is based upon Lin Weiss Bisceglia criteria. The Lin Weiss Bisceglia evaluates some parameters whose presence or absence is indicative of malignancy or benignity. This index classifies tumours in three categories: benign, borderline / uncertain or malignant. Malignancy is defined by the presence of any of the following microscopic features: High mitotic index (rate higher than five per 50 atypical glandular cells), atypical mitosis, or invasion of venous structures. If no criteria of malignancy are present, we should assess if borderline malignancy criteria are applicable. Borderline OAN is diagnosed when one of these microscopic features are present: increased size (>10cm and/or 200g), capsular invasion, sinusoidal invasion or necrosis. Diagnosis of benign OAN is determined when there is no of malignancy signs at all and no more than one borderline criterion is present [1, 3, 6]. According to Weiss criteria, our patient had a borderline OAN. Adrenalectomy is the standard of treatment, and laparoscopy should be performed when there is no evidence of malignancy [2, 7]. Benign OAN has a relatively good prognosis after surgery, but malignant OAN have a survival rate of only 35-50% depending on the invasion rate Borderlin OAN prognosis is uncertain [3, 5].
Consent
Informed consent was obtained from the patient for publication of this case report
Competing Interest
The actors declare that they have no competing interests
Article Info
Article Type
Case ReportPublication history
Received: Mon 25, Feb 2019Accepted: Sat 16, Mar 2019
Published: Sat 30, Mar 2019
Copyright
© 2023 Elena A??n. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.COR.2019.02.001
Author Info
Corresponding Author
Elena A??nDepartment of General Surgery, Hospital Lluís Alcanyís, Spain
Figures & Tables
References
- Harbin A, Chen A, Bhattacharya S, Khurana J, Kaplan J, et al. (2015) Oncocytic Adrenocortical Neoplasm Diagnosed after Robot – Assited Adrenalectomy. Case Rep Urol 2015: 515071.
- Mearini L, Del Sordo R, Costantini E, Nunzi E, Porena M (2013) Adrenal Oncocytic Neoplasm: A Systematic Review. Urol Int 91: 125-133. [Crossref]
- Shenouda M, Brown L, Denning K, Pacioles T (2016) A case of Oncocytic adrenocortical neoplasm of Borderline (Uncertain) Malignant Potential. Cureus 8: e638. [Crossref]
- Chakroun M, Kerkeni W, Zidi Y, Ayed H, Bouzouita A, et al. (2016) Voluminous Incidental Oncocytic Neoplasm of Adrenal Gland with Uncertain Malignant Potential. Urol Case Rep 23: 26-27. [Crossref]
- Corrales JJ, Robles-Lázaro C, Sánchez-Marcos AI, González-Sánchez MC, Antúez-Plaza P, et al. (2016) Plurihormonal Cosecretion by a Case of Adrenocortical Oncocytic Neoplam. Case Reports in Endocrinology 2016: 6785925.
- Wong DD1, Spagnolo DV, Bisceglia M, Havlat M, McCallum D, et al. (2011) Oncocytic adrenocortical neoplasms – a clinicopathologic study of 13 new cases emphasizing the importance of their recognition. Hum Pathol 42: 489-499. [Crossref]
- Del Castillo Déjardin D1, Cabrera Vilanova A1, Vives Espelta M1, Prieto Butillé MR1, Sabench Pereferrer F (2016) Laparoscopic approach in an adrenal right virilizing tumour. Cir Esp 94: 605-607. [Crossref]