A Randomized Trial to Maximize Identification and Genetic Counseling Referral of Women at Risk for Hereditary Breast and Ovarian Cancer
A B S T R A C T
Purpose: The Breast Cancer Genetics Referral Screening Tool (B-RST™) has been endorsed as one of several validated screening tools to identify women appropriate for cancer genetics referral. We conducted a randomized trial to determine the most effective means of follow-up for women who screened positive on B-RST™ 3.0.
Methods: Women undergoing screening mammography at one of four Emory clinics were approached to complete the B-RST™. Participants who screened positive were randomized to one of three follow-up groups: self-referral (Group 1), electronic health record (EHR) clinician messaging (Group 2), or direct contact (Group 3). We compared genetic counseling appointment scheduling and completion rates by group.
Results: Of 2,422 participants, 658 (27.2%) screened positive. Genetic counseling appointments were scheduled by 9.2%, 20.1% and 9.7% of Group 1, 2 and 3 participants respectively (p=0.001). Challenges to scheduling included lack of physician response to EHR messages and unsuccessful direct contact. Among those scheduled (n=78) 70.5% completed the appointment, with no difference between the three groups.
Conclusion: B-RST™ can be used effectively in mammography settings to identify high-risk women for cancer genetics referral. Follow-up via EHR appears an acceptable and efficient approach, but additional strategies are needed to facilitate completion of the genetic counseling process.
Keywords
BRCA1/2, screening tools, genetic counseling, hereditary breast and ovarian cancer
Introduction
Hereditary breast and ovarian cancer syndrome (HBOC) associated with mutations in the BRCA1/2 genes accounts for an estimated 5% of breast cancer and 15% of ovarian cancer [1-3]. For women who carry mutations in these genes, the cumulative risk for breast cancer by age 80 years is 72% for BRCA1 carriers and 69% for BRCA2 carriers. The cumulative risk for ovarian cancer by age 80 years is 44% and 17% for BRCA1 and BRCA2 mutation carriers respectively [4]. While BRCA clinical genetic testing has been available for over 20 years, it is estimated that less than 6% of unaffected carriers and fewer than 20% of carriers with breast and/or ovarian cancer have been identified [5, 6]. This is despite data demonstrating knowledge of mutation status can facilitate early and enhanced screening and preventive surgeries can substantially reduce associated morbidity and mortality [7-9]. Furthermore, cascade testing of at-risk family members can further address the population health impact of HBOC [10]. Offering genetic counseling and testing is common in oncology care, yet identification of unaffected individuals at-risk for HBOC in primary care settings remains problematic [11-13]. Underutilization has been linked to lack of recognition of at-risk individuals and appropriate referral for cancer genetic services [14, 15]. In addition, multiple system and patient barriers to uptake of genetic counseling and testing exist. These include cost, logistical barriers, lack of clinician recommendation, insurance concerns, emotional issues, and low perceived personal relevance [16].
Several studies have reported on identification and/or uptake of genetic counseling for HBOC. These studies vary by the method of identification and follow-up, setting (clinical, research, public health) and target population (affected or unaffected women). Identification of individuals at-risk for HBOC through various protocols has ranged from 2.7% to 13.9% and uptake of genetic counseling from 3% to 50% [17-25]. Application in a research setting, proband history of breast cancer, use of a patient navigator/direct contact, free access to genetic counseling and/or testing, and availability of telephone counseling have resulted in higher rates of uptake [16, 21, 22, 25]. Few studies have focused specifically on prospective identification of unaffected women at risk for HBOC and genetic counseling outcomes in primary care settings in the United States. The 2014 United States Preventive Services Task Force recommendation endorsed screening women at-risk for HBOC for referral to genetic counseling using one of several validated tools [26]. One of the tools highlighted was the Breast Cancer Genetics Referral Screening tool or B-RST™ [27-29]. Previous studies have used the original paper-based (B-)RST, or variations thereof to identify individuals for genetic counseling referral, classify individuals reporting at least one family member with cancer as high-risk and to validate alternate screening tools [22, 30, 31]. A second web-based version of the tool (B-RST™ 2.0) was used in public health clinics [25, 28, 32]. We recently revised and validated B-RST™ Version 3.0, which demonstrated a 94% sensitivity in identifying BRCA mutation carriers [29].
The overall purpose of this project was to prospectively evaluate the implementation of B-RST™ 3.0 in a routine clinical setting. Our primary objective was to identify the most efficient and effective means of follow-up of screen-positive individuals, in order to maximize the number who were referred for, scheduled and completed a cancer genetic counseling appointment. We hypothesized that either direct contact and/or clinician notification via the Electronic Health Record (EHR) would result in more scheduled and completed appointments than self-referral. Our secondary objective was to evaluate utility by analysing the screen-positive rate, and the number seen for genetic counseling who were appropriate for genetic testing, underwent genetic testing and were found to carry a hereditary cancer gene mutation. To our knowledge, this is the first randomized trial performed in a non-public health setting to examine referral methods for individuals identified at increased risk for HBOC.
Materials and Methods
We performed a three-arm parallel intervention randomized clinical trial. The intervention was the method of follow-up for participants who screened positive on B-RST™ 3.0 and included self-referral, clinician notification via EHR messaging, or direct contact. The study was conducted in breast imaging centers at four Emory Healthcare clinics in Atlanta, GA. The study was approved by the Emory University Institutional Review Board. This registered trial can be accessed on (Link 1) (NCT02786147).
I Participants and Recruitment
Eligibility criteria included female patients aged 18 or older presenting for a routine screening mammography between April 2016 and June 2017. Those presenting for a diagnostic mammogram, or any other procedure were excluded. Training of recruiters involved a one-hour session that included background on HBOC, the B-RST™ tool, example scripts and role-play. The PI or study coordinator spent the first day with each recruiter ensuring uniformity of approach. Recruiters provided each prospective participant an overview of the study and a recruitment packet with a pamphlet about HBOC and genetic counseling, and a combined informed consent/HIPAA authorization form. Patients filled out a brief form indicating interest in completing the study. Those who agreed were asked to provide their email address if they were willing to be contacted about related studies. Patients who declined were asked to select a reason. Either before or after completing their mammogram, participants were provided with a tablet opened to a page on a secure browser, which recorded consent electronically.
Participants were not compensated and were informed about insurance coverage and potential costs associated with genetic counseling and testing, should they screen positive. However, these activities were not considered a part of the study, but routine clinical care upon patient referral. Recruitment was continued until the target number of screen-positive individuals as determined by the power calculation was reached.
II Data Collection
Participants self-administered the B-RST™ 3.0 using the tablet. Two demographic questions preceded the first question of the B-RST™ 3.0; level of education and income. All data were saved to a HIPAA compliant database, along with the patient’s medical record number and email address if provided. Demographic data including date of birth, race, and insurance status were abstracted from the EHR. B-RST™ provides three categories of results; screen-positive, screen-negative moderate risk, and screen-negative average risk based on a validated algorithm [29]. Screen “positive” indicates an increased risk for HBOC of at least 5-10%. Screen “negative - moderate risk” indicates a low risk for HBOC, but some increased risk for breast cancer, while screen “negative - average risk” indicates HBOC is very unlikely, and the individual is at average risk for breast and ovarian cancer based on family history. The B-RST™ 3.0 takes approximately 2-5 minutes to complete, depending on the complexity of the family history. Following completion of the tool, the participant was provided with a one-page handout explaining her results and implications, steps for follow-up, information to contact or schedule an appointment with a genetic counselor, and appropriate resource links (Supplementary Materials and Methods-Item1 [SMM-1]). The handout was designed with input from public health, health literacy experts and genetic counselors. We identified the screen-positive rate of B-RST™ 3.0 in this clinical setting and only these participants continued on to the intervention phase.
III Intervention
Screen-positive participants were randomized to one of three types of follow-up for referral/scheduling of cancer genetic counseling. Randomization was one-to-one-to-one and determined by the study coordinator using an online random number generator.
i. Group 1 - Self-Referral: Participants allocated to this group were directed how to schedule a genetic counseling appointment on their own using the contact information provided on the screen-positive handout (SMM-1). However, neither the patient nor the ordering clinician was contacted directly about the B-RST™ 3.0 result or recommendation for genetic counseling.
ii. Group 2: Clinician-Notification: For these participants, the clinician who ordered the mammogram was notified via messaging within the existing EHR system that the patient was at increased risk for HBOC based on their B-RST™ 3.0 result, and that genetic counseling was recommended (SMM-2). The process to order an electronic referral for genetic counseling was provided, as per standard clinic protocol. The electronic referral notifies the Cancer Genetics Program schedulers to contact the patient to arrange the appointment. The schedulers make up to three (phone contact attempts) and leave messages for a return call. A second EHR message was sent to the clinician as a reminder if no referral was made within a month of the first message.
iii. Group 3: Direct Contact: Starting within two weeks after their mammogram appointment, patients in this group received up to five phone calls, an email and/or text messages from a genetic counseling assistant according to the protocol and script provided in SMM-3. If the participant was reached successfully, their positive screening result and the genetic counseling process were explained, family history was verified, and their name and information provided to the schedulers to arrange the appointment if desired.
Participants were followed through December 2017 (six-months after the recruitment of the final participant). The primary outcomes for this study were the number of B-RST™ screen-positive participants in each of the three referral groups who scheduled a cancer genetic counseling appointment, as well as the number who completed the appointment. These data were routinely abstracted from the EHR and/or provided by Emory Winship Cancer Institute Genetic Counseling Program staff. Among participants who completed a genetic counseling appointment, we determined the number who were offered genetic testing for either themselves or a family member, underwent genetic testing, and test results. These secondary outcomes were obtained from review of genetic counseling clinic notes. The genetic counseling and testing occurred through standard in-person clinical services provided by board certified genetic counselors at three Emory Winship Cancer Institute sites in metro Atlanta. These sessions were not conducted as part of the study protocol. Wait-time to access these services averages less than two weeks. Data regarding average non-completion of regularly scheduled genetic counseling appointments were ascertained, as well as zip codes of the participants to address the issue of travel as a barrier.
IV Statistical Analyses
We estimated that 10% of women who screened positive with no direct follow-up (self-referral group) would schedule a cancer genetic counseling appointment. Setting power at 80% and alpha at 0.05, we calculated that 200 participants in each group would be required to see a difference of at least 20% in scheduling rates. Demographic variables (age, race, education, household income, and insurance) were examined in relation to study condition (referral group) and both of the main study outcomes (scheduled appointment, completed appointment) using Chi-square analyses. Differences in the proportion of participants who scheduled and completed genetic counseling appointments among the three groups were also evaluated using Chi-square. Fisher’s exact was used to determine if completion of scheduled appointments differed by study condition. Odds ratios of scheduling and completing genetic counseling were calculated with simple logistic regression, as adjustment for demographic variables was not required. In addition to the intent-to-treat analysis, we evaluated the primary outcomes after removing individuals whose clinician never forwarded the EHR message to scheduling, or who we were unable to reach by direct contact (treatment per protocol). All analyses were completed using SPSS version 24, with the threshold for statistical significance set at α=0.05.
Results
Figure 1 illustrates study participation and main outcomes. Of the 3,865 women approached, 2,422 (62.7%) participated. We compared race and age groups of our participants to that of the overall mammography population during the same time period. There was no difference by race, though fewer participants were age 70 (16.9% vs. 22.3%, p<0.0001). Of those providing a reason for non-participation (n=869) the most common were: lack of time (34.3%), no perceived benefit (20.4%), privacy concerns (9.9%), no family history (8.4%) and cancer worry (7.1%). Of the 2,442 participants, 658 (27.2%) screened positive, and were randomized to follow-up. Screen-positive rates did not differ by race, age, education or income (data not shown). A total of 50 screen-positives (7.6%) had previously undergone genetic counseling and/or testing and were eliminated from further analysis. Figure 1 also illustrates the outcomes of attempted EHR notification of clinicians and direct contact of patients. Figure S1 provides the CONSORT flow diagram [33].
Table 1: Screen-positive participant demographics.
|
Total Screen
Positives (n=658) |
Scheduled Appointment n (% of 78) |
P valuea |
Completed Appointment n (% of 55) |
P valuea |
|
|
Age in years |
0.905 |
0.833 |
|||
|
<40 |
11 (1.7) |
1 (1.3) |
1 (1.8) |
||
|
40-69 |
539 (81.9) |
63 (80.8) |
43 (78.2) |
||
|
≥70 |
108 (16.4) |
14 (17.9) |
11 (20.0) |
||
|
Race |
0.424 |
0.021 |
|||
|
White |
329 (50.0) |
44 (56.4) |
37 (67.3) |
||
|
Black |
278 (42.2) |
30 (38.5) |
14 (25.5) |
||
|
Other |
51 (7.8) |
4 (5.1) |
|
4 (7.3) |
|
|
Educationb |
n=642 |
n=77 |
0.445 |
0.192 |
|
|
High school or less |
62 (9.7) |
7 (9.1) |
6 (10.9) |
||
|
Some college |
144 (22.4) |
13 (16.9) |
7 (12.7) |
||
|
College/prof degree |
436 (67.9) |
57 (74.0) |
42 (76.4) |
||
|
Incomeb |
n=562 |
n=61 |
0.740 |
n=41 |
0.445 |
|
$25,000 or less |
54 (9.6) |
5 (8.2) |
3 (7.3) |
||
|
$25,001 to $50,000 $50,001 to $75,000 |
81 (14.4) 125 (22.2) |
8 (13.1) 17 (27.9) |
4 (9.8) 13 (31.7) |
||
|
$75,001 or more |
302 (53.7) |
31 (50.8) |
21 (51.2) |
||
|
Insurance Type |
|
0.798 |
|
0.626 |
|
|
Private/employer based |
355 (54.0) |
41 (52.6) |
|
27 (49.1) |
|
|
Medicaid/Medicare |
121 (18.4) |
17 (21.8) |
12 (21.8) |
||
|
Self-Pay |
20 (3.0) |
3 (3.8) |
3 (5.5) |
||
|
Unknown |
162 (24.6) |
17 (21.8) |
13 (23.6) |
aChi-square and Fisher’s exact (n<5).
bParticipant totals less than number enrolled due to
missing data.
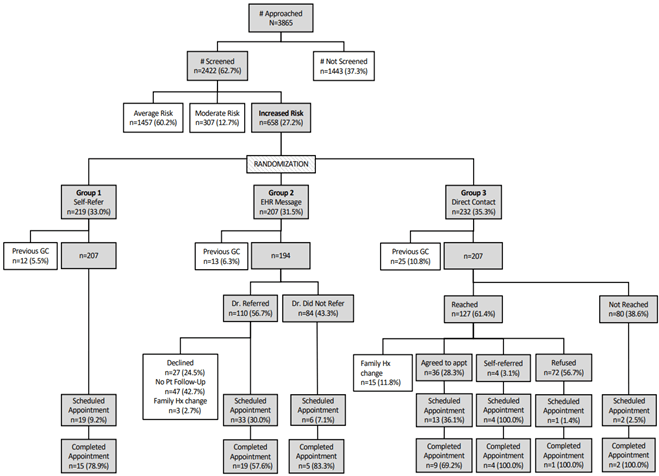
Figure 1: Study flowchart.
Appt: Appointment; GC: Genetic Counseling; Hx: History; Pt: Patient.
Table 1 shows the demographics of the screen-positive participants. Half of the study participants were white (50.0%) and 42.2% were black. The majority were between the ages of 40-69 (81.9%), had a college or professional degree (67.9%) and had incomes greater than $75,000 (53.7%). Demographics did not differ by study group, demonstrating effective randomization. There were also no differences in any demographic variables between screen-positive individuals who scheduled an appointment and those who did not. The frequency of completion differed only by race, with black and other race participants significantly less likely to complete genetic counseling than white participants (p=0.02).
Table 2: Genetic counseling
appointments by study condition (intent to treat).
|
Self-referral (Group
1) n=207 |
EHR Message (Group
2) n=194 |
Direct Contact (Group
3) n=207 |
Total n=608a |
P valueb |
|
|
|
|
n (% of group) |
|
|
|
|
Scheduled Appointment |
19 (9.2) |
39 (20.1) |
20 (9.6) |
78 (12.8) |
0.001 |
|
Completed Appointment |
15 (7.2) |
24 (12.4) |
16 (7.7) |
55 (9.0) |
0.145 |
|
% Completed of Scheduled |
78.9% |
61.5% |
80.0% |
70.5% |
0.220 |
aParticipants having had previous genetic counseling (n=50) removed; bP
value based on Chi-square test.
Table 3: Likelihood of scheduling and completing genetic counseling appointment.
|
|
Group 2 vs. 1 |
Group 2 vs. 3 |
Group 3 vs. 1 |
|
|
OR (95% CI) |
||||
|
Intent to Treat (n=608) |
|
|||
|
Scheduled Appointment |
2.49 (1.38, 4.48) |
2.35 (1.32,
4.20) |
1.10 (0.55, 2.05) |
|
|
Completed Appointment |
1.81 (0.92, 3.56) |
1.68 (0.87, 1.14) |
1.07 (0.52, 2.23) |
|
|
Received Intervention (n=444) |
|
|
|
|
|
Scheduled Appointment |
4.24 (2.27, 7.9) |
2.60 (1.36,
4.95) |
1.63 (0.82, 3.25) |
|
|
Completed Appointment |
2.67 (1.3, 5.5) |
1.68 (0.80, 3.55) |
1.59 (0.74, 3.41) |
|
Table 4: Genetic counseling appointments by study condition (received
intervention).
|
Self-referral (Group 1) n=207 |
EHR Message (Group 2) n=110 |
Direct Contact (Group 3) n=127 |
Total n=444 |
P valuea |
|
|
|
|
n (% of group) |
|
|
|
|
Scheduled Appointment |
19 (9.2) |
33 (30.0) |
18 (14.1) |
70 (15.8) |
< 0.0001 |
|
Completed Appointment |
15 (7.2) |
19 (17.2) |
14 (11.0) |
48 (10.8) |
0.024 |
|
% Completed of Scheduled |
78.9% |
57.6% |
77.8% |
68.6% |
0.173 |
Of the 608 screen-positive participants analysed per intent-to-treat, 78 (12.8%) scheduled a genetic counseling appointment by the end of the study follow-up period (Table 2). Those in Group 2 (EHR message) were significantly more likely to schedule (20.1%) compared to those in Groups 1 (self-referral) and 3 (direct contact) at 9.2% and 9.6% respectively, p<0.001. Individuals in Group 2 were 2.49 times (95% CI 1.4-4.5) more likely to schedule than those in Group 1, and 2.35 times (95% CI 1.3-4.2) more likely than those in Group 3 (Table 3). A total of 55 (9.0%) of randomized screen-positive participants completed genetic counseling, with no difference by group in the rate of completion of scheduled appointments (overall 70.5%). This rate of completion of scheduled appointments is lower than the 80-85% obtained from routine clinic data. The average estimated distance to the primary Winship Genetic Counseling Program location was 14 miles based on participant zip-codes, excluding six individuals from out-of-state.
Among the screen-positive participants (n=608), 444 (73%) received the per-protocol intervention (Table 4). In this analysis, a total of 70 participants (15.8%) scheduled a genetic counseling appointment. Those in Group 2 again had the highest scheduling rate (30.0%), differing significantly from both Group 1 (9.2%) and Group 3 (14.1%), p<0.0001. The odds ratios for scheduling genetic counseling (among those who received the per-protocol intervention) in Group 2 compared to Groups 1 and 3 were 4.24 (95% CI 2.27-7.91) and 2.6 (95% CI 1.36-4.95), respectively (Table 3). Group 2 participants were also more likely to have completed a genetic counseling appointment (17.2%) when receiving the intended intervention (p=0.02). A majority (n=48) of the screen-positive participants who completed cancer genetic counseling (n=55) were offered genetic testing in themselves or a family member. The remaining seven participants were not offered testing due to previous negative BRCA testing in the family (n=2), failure to meet specific insurance criteria (n=2), and not considered high-risk on clarification of family history (n=3). Excluding those whose family history changed upon direct genetic counseling inquiry, 52 of 55 (94.5%) were considered appropriate for genetic testing. Of the 37 participants who were themselves offered genetic testing, 21 (56.8%) completed the process. The remaining patients were still considering (n=7), did not have insurance that would cover testing (n=5), or did not want to undergo testing (n=4). Variants were identified in six individuals, of which three were considered pathogenic: one in BRCA2, one in ATM and one in CHEK2. The remaining three (one each in PALB2, FANCC, APC) were classified as variants of uncertain significance.
Discussion
There is broad consensus of the benefits of genetic counseling and testing of individuals at-risk for HBOC [11, 26, 34]. Unfortunately, a majority of those most at-risk have yet to be identified either due to lack of clinician recognition, or poor uptake of cancer genetic counseling and testing [5, 6]. B-RST™ was developed and validated to facilitate the identification and referral of individuals at-risk for HBOC. This brief questionnaire, available online at (Link 2), is highly sensitive for identifying individuals who should be referred for cancer genetic services [27-29].
We administered B-RST™ 3.0 using a tablet among women presenting for screening mammography with the goal of identifying if informed self-referral, EHR messaging to the ordering clinician, or direct patient contact resulted in the highest rate of scheduling and uptake of cancer genetic services. Our results suggest that administration of B-RST™ via tablet is feasible in a busy mammography clinic, with reasonable interest and participation rates in a study setting. Among those identified at increased risk for HBOC (27.2%), the overall frequency of genetic counseling scheduling and completion was 15.8% and 10.8% respectively in the per-protocol analysis. While EHR messaging of the ordering clinician was found to be the most effective method of referral for both scheduling (30.0%) and uptake (17.2%) of genetic counseling, these rates remain less than ideal. However, our uptake rate was not dissimilar from that reported in previous studies 3% to 50% [17-25]. While overall uptake was low, only 8% of screen-positive participants had previously received genetic counseling, suggesting a substantial increase in the identification of at-risk individuals.
We believe that lack of direct communication between the patient and clinician regarding the screen-positive result may have influenced outcomes. Scheduling rates were 30% when the clinician responded to the EHR message by forwarding the patient information to the Cancer Genetics scheduling staff as recommended, compared to 7% when he/she did not. However, if the clinician had the opportunity to discuss the B-RST™ result with the participant, it is likely that uptake would have increased. In follow-up qualitative interviews with individuals who did not complete genetic counseling, Kne et al. found that women desired a discussion with their clinician and a recommendation that they seek cancer genetic services [18]. Other studies have demonstrated the importance of clinician recommendation in maximizing utilization of genetic counseling and testing [35, 36]. To reflect a real-world setting however, we chose to follow the routine clinical protocol, where patients are referred for genetic counseling by the clinician sending the patient information to schedule via the EHR.
Previous studies have also shown less than ideal uptake of cancer genetic services among unaffected women who screened as high-risk [18, 21-23]. With respect to method of follow-up, patient contact via letter seems to result in lower levels of uptake than direct patient contact by a trained individual [18, 21-23]. To our knowledge, only one prior study randomized screen-positive individuals to alternate types of follow-ups. Pasick et al. screened 1212 women calling in to a public health breast and cervical cancer telephone service. Among the individuals identified at high-risk (14%), 39% of those randomized to direct contact with an immediate offer of free genetic counseling received services, vs. 4.5% of those receiving a brochure [21]. It is likely that the immediate offer of a free service, vs. notifying the scheduler in accordance with our clinical protocols, influenced these higher uptake rates.
Another factor that likely affected uptake was the lack of availability of telephone genetic counseling in our system at the time. Paris et al. found an uptake rate of 67% when patients were contacted by a genetic nurse specialist who provided telephone consultation [25]. Pasik et al. found increased uptake of genetic counseling when telephone counseling was offered compared to in-person only [21]. While travel was not likely a large barrier in our case given the average distance to cancer genetic services was 14 miles, the convenience of telecounseling may have resulted in higher uptake. Several studies have suggested both outcome equivalency (knowledge and satisfaction) and patient preference for telephone genetic counseling over in-person genetic counseling [37].
Robinson et al. reported one of the largest clinical HBOC screening projects to date [22]. A modified version of the original paper-based (B-)RST was administered to 61,294 underserved women and 24,131 insured women undergoing screening mammography. The underserved cohort received direct contact from a patient navigator, resulting in 51% obtaining a referral to genetics, with half of these completing the appointment. For the insured cohort, high-risk status was noted in the mammography report, and only 13% received a clinician referral to genetics, though 85% completed the appointment. In contrast, we saw a higher referral rate (56.7%) with clinician notification via EHR messaging in our mostly insured cohort, and a lower completion rate of scheduled appointments (57.6%), which was not significantly different from the completion rate in the self-referral or the direct contact groups.
These past studies suggest that uptake among the underserved may be substantially enhanced by direct contact and assistance with scheduling and follow-through. Whether our method of EHR messaging to the ordering clinician, vs. notification via mammography report results in differential uptake requires investigation. Our results indicate direct contact may not be more effective in a mostly insured population. Given that direct patient contact requires significantly more resources with respect to time and personnel, we suggest that automated EHR messaging and email follow-up to the patient may be the most effective and efficient approach for insured populations. The B-RST™ 3.0 screen-positive rate of 27.2% in this study is substantially higher than the 5-6% found with the earlier versions [22, 27, 32]. There are several potential explanations for this, including the changes made to increase the sensitivity of the B-RST™ 3.0 version, the mammography setting, selective participation of those at increased risk, and an older cohort (mean age 58.4 years, SD=10.8) [29]. The higher screen-positive rate is consistent with the broader criteria for HBOC counseling and testing put forth by the National Comprehensive Cancer Network [38].
While our 63% participation rate was less than preferred, it is reasonable for a non-incentivized study in this type of setting. Our results are limited by the lack of complete demographic data of non-participants. However, in comparison to the general mammography population, there was no difference in participation by race, and by age it differed only in the 70 years category. The primary reason for non-participation of “I do not have time to participate”, would be eliminated if completing B-RST™ became a routine clinical practice. Generalizability of this study is limited by our mostly insured, educated and higher SES participant population. However, over 40% of participants were black, indicating these findings are likely relevant to this insured sub-population, especially as participation did not differ by race. We suspect there was some participation bias that may have skewed the screening outcomes, particularly the proportion who screened positive or negative-moderate. This is supported by the finding that 8.4% of non-participants reported “no family history” as the reason for non-participation. Another limitation of our study is the relatively low number of screen-positive individuals who completed genetic counseling and testing, as it precluded meaningful conclusions regarding the clinical utility of B-RST™ in terms of identifying mutation carriers. However, the fact that 95% of those who pursued genetic counseling were considered appropriate for genetic testing, in themselves or a family member, demonstrates utility with respect to identification of at-risk individuals. Strengths of our study include application in a real clinical setting, the overall number of participants, the effectiveness of randomization, the depth of follow-up, and racial diversity.
As the results of this study suggest that screening with B-RST™ 3.0 in mammography settings is feasible, and that notification of the ordering clinician via EHR maximizes scheduling rates, implementation as routine clinical care should be considered in insured populations. Pre-education of ordering clinicians and their staff about B-RST™ 3.0 and screen-positive implications, as well as email (or patient portal) contact with individuals who do not schedule genetic counseling would be expected to maximize uptake. This follow-up could be automated within the EHR system to increase efficiency. To eliminate patients being scheduled who may have completed the tool incorrectly, we would suggest a brief conversation with the patient prior to the appointment to confirm the family history reported. Such follow-up could be conducted by genetic counseling assistants who are increasingly used in this manner to maximize the time genetic counselors have to see patients [39]. Future studies should evaluate implementation via primary care clinicians, for example at routine annual physicals. B-RST™ 3.0 could be completed by a nurse or medical assistant or self-administered by the patient. The clinician would see the result immediately, be able to talk in real-time with the patient about the implications and make a direct referral to genetic counseling during the visit.
There remains a need to identify individuals at risk for HBOC for referral to genetic services. Use of B-RST™ 3.0 as a screening tool in mammography with EHR follow-up, and potentially in primary care settings, could increase the number of at-risk individuals who receive these services. However, until barriers to uptake of genetic counseling and testing are addressed at a systems and population level, there will remain underutilization of these services and therefore missed opportunities to improve public health using this personalized medicine approach.
Acknowledgement
The research in this publication was supported in part by a grant from the Brenda Nease Breast Cancer Research Fund Award/Winship Cancer Institute of Emory University along with Winship Cancer Institute NCI/NIH funding (P30CA138292) and Winship Core Facilities including - the Intervention Development, Dissemination and Implementation Developing Shared Resource and the Biostatistics and Bioinformatics Shared Resource. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Article Info
Article Type
Research ArticlePublication history
Received: Fri 22, Jan 2021Accepted: Wed 18, Aug 2021
Published: Tue 31, Aug 2021
Copyright
© 2023 Cecelia Bellcross. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.COR.2021.08.08
Figures & Tables
Table 1: Screen-positive participant demographics.
|
Total Screen
Positives (n=658) |
Scheduled Appointment n (% of 78) |
P valuea |
Completed Appointment n (% of 55) |
P valuea |
|
|
Age in years |
0.905 |
0.833 |
|||
|
<40 |
11 (1.7) |
1 (1.3) |
1 (1.8) |
||
|
40-69 |
539 (81.9) |
63 (80.8) |
43 (78.2) |
||
|
≥70 |
108 (16.4) |
14 (17.9) |
11 (20.0) |
||
|
Race |
0.424 |
0.021 |
|||
|
White |
329 (50.0) |
44 (56.4) |
37 (67.3) |
||
|
Black |
278 (42.2) |
30 (38.5) |
14 (25.5) |
||
|
Other |
51 (7.8) |
4 (5.1) |
|
4 (7.3) |
|
|
Educationb |
n=642 |
n=77 |
0.445 |
0.192 |
|
|
High school or less |
62 (9.7) |
7 (9.1) |
6 (10.9) |
||
|
Some college |
144 (22.4) |
13 (16.9) |
7 (12.7) |
||
|
College/prof degree |
436 (67.9) |
57 (74.0) |
42 (76.4) |
||
|
Incomeb |
n=562 |
n=61 |
0.740 |
n=41 |
0.445 |
|
$25,000 or less |
54 (9.6) |
5 (8.2) |
3 (7.3) |
||
|
$25,001 to $50,000 $50,001 to $75,000 |
81 (14.4) 125 (22.2) |
8 (13.1) 17 (27.9) |
4 (9.8) 13 (31.7) |
||
|
$75,001 or more |
302 (53.7) |
31 (50.8) |
21 (51.2) |
||
|
Insurance Type |
|
0.798 |
|
0.626 |
|
|
Private/employer based |
355 (54.0) |
41 (52.6) |
|
27 (49.1) |
|
|
Medicaid/Medicare |
121 (18.4) |
17 (21.8) |
12 (21.8) |
||
|
Self-Pay |
20 (3.0) |
3 (3.8) |
3 (5.5) |
||
|
Unknown |
162 (24.6) |
17 (21.8) |
13 (23.6) |
aChi-square and Fisher’s exact (n<5).
bParticipant totals less than number enrolled due to
missing data.
Table 2: Genetic counseling
appointments by study condition (intent to treat).
|
Self-referral (Group
1) n=207 |
EHR Message (Group
2) n=194 |
Direct Contact (Group
3) n=207 |
Total n=608a |
P valueb |
|
|
|
|
n (% of group) |
|
|
|
|
Scheduled Appointment |
19 (9.2) |
39 (20.1) |
20 (9.6) |
78 (12.8) |
0.001 |
|
Completed Appointment |
15 (7.2) |
24 (12.4) |
16 (7.7) |
55 (9.0) |
0.145 |
|
% Completed of Scheduled |
78.9% |
61.5% |
80.0% |
70.5% |
0.220 |
aParticipants having had previous genetic counseling (n=50) removed; bP
value based on Chi-square test.
Table 3: Likelihood of scheduling and completing genetic counseling appointment.
|
|
Group 2 vs. 1 |
Group 2 vs. 3 |
Group 3 vs. 1 |
|
|
OR (95% CI) |
||||
|
Intent to Treat (n=608) |
|
|||
|
Scheduled Appointment |
2.49 (1.38, 4.48) |
2.35 (1.32,
4.20) |
1.10 (0.55, 2.05) |
|
|
Completed Appointment |
1.81 (0.92, 3.56) |
1.68 (0.87, 1.14) |
1.07 (0.52, 2.23) |
|
|
Received Intervention (n=444) |
|
|
|
|
|
Scheduled Appointment |
4.24 (2.27, 7.9) |
2.60 (1.36,
4.95) |
1.63 (0.82, 3.25) |
|
|
Completed Appointment |
2.67 (1.3, 5.5) |
1.68 (0.80, 3.55) |
1.59 (0.74, 3.41) |
|
Table 4: Genetic counseling appointments by study condition (received
intervention).
|
Self-referral (Group 1) n=207 |
EHR Message (Group 2) n=110 |
Direct Contact (Group 3) n=127 |
Total n=444 |
P valuea |
|
|
|
|
n (% of group) |
|
|
|
|
Scheduled Appointment |
19 (9.2) |
33 (30.0) |
18 (14.1) |
70 (15.8) |
< 0.0001 |
|
Completed Appointment |
15 (7.2) |
19 (17.2) |
14 (11.0) |
48 (10.8) |
0.024 |
|
% Completed of Scheduled |
78.9% |
57.6% |
77.8% |
68.6% |
0.173 |
Appt: Appointment; GC: Genetic Counseling; Hx: History; Pt: Patient.
References
1.
Risch
HA, McLaughlin JR, Cole DEC, Rosen B, Bradley L et al. (2006) Population BRCA1
and BRCA2 mutation frequencies and cancer penetrances: a kin-cohort study in
Ontario, Canada. J Natl Cancer Inst 98:
1694-1706. [Crossref]
2.
Anglian
Breast Cancer Study Group (2000) Prevalence and penetrance of BRCA1 and BRCA2
mutations in a population-based series of breast cancer cases. Anglian Breast
Cancer Study Group. Br J Cancer 83:
1301-1308. [Crossref]
3.
Maxwell
KN, Domchek SM, Nathanson KL, Robson ME (2016) Population Frequency of Germline
BRCA1/2 Mutations. J Clin Oncol 34:
4183-4185. [Crossref]
4.
Kuchenbaecker
KB, Hopper JL, Barnes DR, Phillips KA, Mooij TM et al. (2017) Risks of Breast,
Ovarian, and Contralateral Breast Cancer for BRCA1 and BRCA2 Mutation Carriers.
JAMA 317: 2402-2416. [Crossref]
5.
Drohan
B, Roche CA, Cusack Jr JC, Hughes KS (2012) Hereditary breast and ovarian
cancer and other hereditary syndromes: using technology to identify carriers. Ann Surg Oncol 19: 1732-1737. [Crossref]
6.
Childers
CP, Childers KK, Maggard Gibbons M, Macinko J (2017) National Estimates of
Genetic Testing in Women With a History of Breast or Ovarian Cancer. J Clin Oncol 35: 3800-3806. [Crossref]
7.
Domchek
SM, Friebel TM, Singer CF, Evans DG, Lynch HT et al. (2010) Association of
risk-reducing surgery in BRCA1 or BRCA2 mutation carriers with cancer risk and
mortality. JAMA 304: 967-975. [Crossref]
8.
Finch
APM, Lubinski J, Møller P, Singer CF, Karlan B et al. (2014) Impact of
oophorectomy on cancer incidence and mortality in women with a BRCA1 or BRCA2
mutation. J Clin Oncol 32: 1547-1553.
[Crossref]
9.
Li
X, You R, Wang X, Liu C, Xu Z et al. (2016) Effectiveness of Prophylactic
Surgeries in BRCA1 or BRCA2 Mutation Carriers: A Meta-analysis and Systematic
Review. Clin Cancer Res 22:
3971-3981. [Crossref]
10.
George
R, Kovak K, Cox SL (2015) Aligning policy to promote cascade genetic screening
for prevention and early diagnosis of heritable diseases. J Genet Couns 24: 388-399. [Crossref]
11.
Robson
ME, Bradbury AR, Arun B, Domchek SM, Ford JM et al. (2015) American Society of
Clinical Oncology Policy Statement Update: Genetic and Genomic Testing for
Cancer Susceptibility. J Clin Oncol 33:
3660-3667. [Crossref]
12.
Bellcross
CA, Kolor K, Goddard KAB, Coates RJ, Reyes M et al. (2011) Awareness and
utilization of BRCA1/2 testing among U.S. primary care physicians. Am J Prev Med 40: 61-66. [Crossref]
13.
Trivers
KF, Baldwin LM, Miller JW, Matthews B, Andrilla CHA et al. (2011) Reported
referral for genetic counseling or BRCA 1/2 testing among United States
physicians: A vignette-based study. Cancer
117: 5334-5343. [Crossref]
14.
Levy
DE, Garber JE, Shields AE (2009) Guidelines for genetic risk assessment of
hereditary breast and ovarian cancer: early disagreements and low utilization. J Gen Intern Med 24: 822-828. [Crossref]
15.
Bellcross
CA, Leadbetter S, Alford SH, Peipins LA (2013) Prevalence and healthcare
actions of women in a large health system with a family history meeting the 2005
USPSTF recommendation for BRCA genetic counseling referral. Cancer Epidemiol Biomarkers Prev 22:
728-735. [Crossref]
16.
Willis
AM, Smith SK, Meiser B, Ballinger ML, Thomas DM et al. (2017) Sociodemographic,
psychosocial and clinical factors associated with uptake of genetic counselling
for hereditary cancer: a systematic review. Clin
Genet 92: 121-133. [Crossref]
17.
Flória Santos M, Lopes Júnior LC, de
Mello Alvarenga L, Ribeiro MS, de Faria Ferraz VE et al. (2016) Self-reported cancer family
history is a useful tool for identification of individuals at risk of
hereditary cancer predisposition syndrome at primary care centers in
middle-income settings: a longitudinal study. Genet Mol Biol 39: 178-183. [Crossref]
18.
Kne
A, Zierhut H, Baldinger S, Swenson KK, Mink P et al. (2017) Why Is Cancer
Genetic Counseling Underutilized by Women Identified as at Risk for Hereditary
Breast Cancer? Patient Perceptions of Barriers Following a Referral Letter. J Genet Couns 26: 697-715. [Crossref]
19.
Ayme A, Viassolo V, Rapiti E, Fioretta
G, Schubert H et al. (2014)
Determinants of genetic counseling uptake and its impact on breast cancer
outcome: a population-based study. Breast
Cancer Res Treat 144: 379-389. [Crossref]
20.
Westman
J, Hampel H, Bradley T (2000) Efficacy of a touchscreen computer based family
cancer history questionnaire and subsequent cancer risk assessment. J Med Genet 37: 354-360. [Crossref]
21.
Pasick
RJ, Joseph G, Stewart S, Kaplan C, Lee R et al. (2016) Effective Referral of
Low-Income Women at Risk for Hereditary Breast and Ovarian Cancer to Genetic
Counseling: A Randomized Delayed Intervention Control Trial. Am J Public Health 106: 1842-1848. [Crossref]
22.
Robinson
LS, Hendrix A, Xie XJ, Yan J, Pirzadeh Miller S et al. (2015) Prediction of
Cancer Prevention: From Mammogram Screening to Identification of BRCA1/2
Mutation Carriers in Underserved Populations. EBioMedicine 2: 1827-1833. [Crossref]
23.
Mays
D, Sharff ME, DeMarco TA, Williams B, Beck B et al. (2012) Outcomes of a
systems-level intervention offering breast cancer risk assessments to low-income
underserved women. Fam Cancer 11:
493-502. [Crossref]
24.
Ashton Prolla P, Giacomazzi J, Schmidt
AV, Roth FL, Palmero EI et al. (2009) Development and validation of a simple questionnaire for the
identification of hereditary breast cancer in primary care. BMC Cancer 9: 283. [Crossref]
25.
Paris
NM (2016) Hereditary breast and ovarian cancer: risk assessment in minority
women and provider knowledge gaps. J
Commun Support Oncol 14: 261-267.
26.
Moyer
VA, U.S. Preventive Services Task Force (2014) Risk assessment, genetic
counseling, and genetic testing for BRCA-related cancer in women: U.S.
Preventive Services Task Force recommendation statement. Ann Intern Med 160: 271-281. [Crossref]
27.
Bellcross
CA, Lemke AA, Pape LS, Tess AL, Meisner LT (2009) Evaluation of a
breast/ovarian cancer genetics referral screening tool in a mammography
population. Genet Med 11: 783-789. [Crossref]
28.
Bellcross
C (2010) Further development and evaluation of a breast/ovarian cancer genetics
referral screening tool. Genet Med 12:
240. [Crossref]
29.
Bellcross
C, Hermstad A, Tallo C, Stanislaw C (2019) Validation of Version 3.0 of the
Breast Cancer Genetics Referral Screening Tool (B-RST). Genet Med 21: 181-184. [Crossref]
30.
Solomon
BL, Whitman T, Wood ME (2016) Contribution of extended family history in
assessment of risk for breast and colon cancer. BMC Fam Pract 17: 126. [Crossref]
31.
Stewart
SL, Kaplan CP, Lee R, Joseph G, Karliner L et al. (2016) Validation of an
Efficient Screening Tool to Identify Low-Income Women at High Risk for
Hereditary Breast Cancer. Public Health
Genomics 19: 342-351. [Crossref]
32.
Brannon
Traxler L, Martin ML, Kerber AS, Bellcross CA, Crane BE et al. (2014) Implementing
a screening tool for identifying patients at risk for hereditary breast and
ovarian cancer: a statewide initiative. Ann
Surg Oncol 21: 3342-3347. [Crossref]
33.
Schulz
KF, Altman DG, Moher D, CONSORT Group (2010) CONSORT 2010 statement: updated
guidelines for reporting parallel group randomised trials. BMJ 340: c332. [Crossref]
34.
Practice
Bulletin No. 182 Summary: Hereditary Breast and Ovarian Cancer Syndrome (2017) Obstet Gynecol 130: 657-659. [Crossref]
35.
Anderson
B, McLosky J, Wasilevich E, Lyon Callo S, Duquette D et al. (2012) Barriers and
facilitators for utilization of genetic counseling and risk assessment services
in young female breast cancer survivors. J
Cancer Epidemiol 2012: 298745. [Crossref]
36.
Chin
TM, Tan SH, Lim SE, Lau P, Yong WP et al. (2005) Acceptance, motivators, and
barriers in attending breast cancer genetic counseling in Asians. Cancer Detect Prev 29: 412-418. [Crossref]
37.
McCuaig
JM, Armel SR, Care M, Volenik A, Kim RH et al. (2018) Next-Generation Service
Delivery: A Scoping Review of Patient Outcomes Associated with Alternative
Models of Genetic Counseling and Genetic Testing for Hereditary Cancer. Cancers (Basel) 10: 435. [Crossref]
38. National Comprehensive Cancer Network (2017) NCCN Clinical Practice Guidelines in Oncology: Genetic/Familial High-Risk Assessment: Breast and Ovarian. Version 1.
39. Pirzadeh Miller S, Robinson LS, Read P, Ross TS (2017) Genetic Counseling Assistants: an Integral Piece of the Evolving Genetic Counseling Service Delivery Model. J Genet Couns 26: 716-727. [Crossref]