Journals
A 6 years follow-up comparison of two dental implants: bioactive vs DAE surface, a clinical case report
A B S T R A C T
Introduction: The aim of the present study is to describe a case report of lower molars substitution with 2 different dental implants. One with a DAE surface and one with a type 1 collagen coated surface.
Case presentation: In the present study, a 54-year-old man presented the absence of the first and second molars both on the left and on the right mandible. After clinical and radiographic evaluation, implant therapy was chosen to substitute the missing teeth. On the right mandible, a DAE surface implant was placed while on the left mandible, a bovine Type 1 collagen of dermal origin (custom made medical device) surface implant was placed. A radiographic 6 years follow up was performed.
Discussion: The Type 1 collagen coated surface dental implant did not show any marginal bone loss after 6 years, moreover, it showed a bone gain after 3 months from its placement and kept it for 6 years while the traditional surface implant showed an immediate marginal bone loss.
K E Y W O R D S
Dental implants, type 1 Collagen, bioactive surface
Abbreviations
DAE: dual acid-etched surface
BIC: Bone Implant Contact
Tb. Th: trabecular thickness
I N T R O D U C T I O N
Dental implant supported prosthesis represents a highly successful and diffused therapy to replace missing teeth [1]. Nowadays, a common implant surface used is the “DAE”, a physical modification, made by acid etching the implant titanium surface [2, 3]. Success rate of this kind of dental implants is high and varies between 82.7% and 98.8% in healthy adult patients [4]. However, this rate decreases dramatically when implants are positioned in “bad quality” bone, which can be found in a precise anatomic district such as the tuber maxillae, regenerated bone and post extractive sites [5-7]. Indeed, the need for enhanced dental implant survival at sites of lower bone density has stimulated researchers to study new implant surface designs and modifications with the purpose to make molecules that play an important role in bone formation, available exactly where they are needed, that is, the bone-implant interface. These new surfaces are created by both physical and biochemical modifications, coating titanium with biologically active molecules such as peptides, ECM proteins or growth factors [8-9]. Between them, animal Type 1 collagen showed promising results when used as a coating material for etched titanium surfaces [10, 11]. Type I collagen constitutes the largest organic portion of the bone, and in regeneration processes, osteoblastic cells initially deposit a collagen matrix which is subsequently mineralized. This collagen matrix has many positive biological effects in bone formation, such as facilitating cell adhesion of osteoblasts and osteoclasts, acting as a co-factor for numerous growth factors, modulating the expression of membrane receptors [12-14]. Thus, the presence of a collagen matrix around the titanium implant would anticipate the first stages of bone formation, presenting a matrix ready to be mineralized by the osteoblasts and providing a biochemical stimulation at the same time [15]. The present case report describes a 6-year follow-up comparison between two titanium dental implants positioned in the same patient; 1 implant had a “DAE” surface and 1 implant had a “DAE” surface and was Type I collagen coated.
Figures
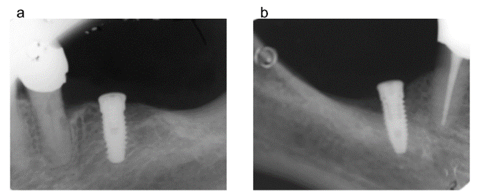
Figure 1: radiographs taken immediately after surgery: DAE surface implant placed at the crestal bone level (Fig. 1a), distal bone around the collagen coated implant is partially missing (Fig.1b)
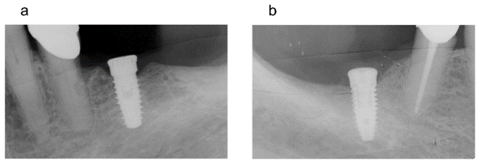
Figure 2: 3 months follow up radiographs: slight periimplant crestal bone resorption around the DAE surface dental implant (Figure 2a), bone quantity increases around the collagen coated implant until covering the head of the implant (Figure 2b).
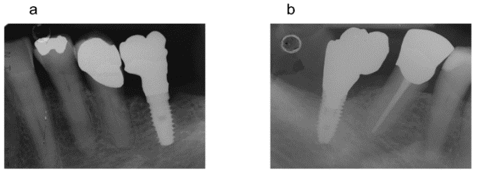
Figure 3: 12 months follow up radiographs: bone resorption is unchanged around the DAE surface dental implant (Fig. 3a) bone quantity increase is maintained around the collagen coated implant (Fig 3b).
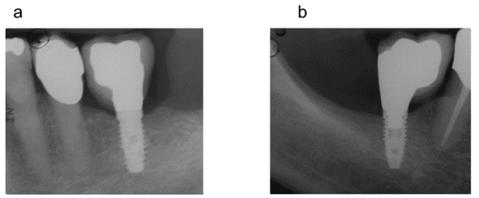
Figure 4: 6 years follow up radiographs: the radiographic bone situation is unchanged both for the the DAE surface dental implant (Fig. 4a) and for the collagen coated implant (Fig. 4b).

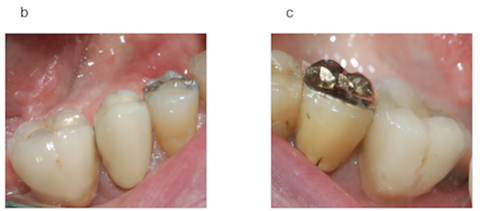
Figure 5: Clinical situation at the 6 years follow up (Figure 5a); DAE surface implant supported crown (Figure 5b); collagen coated implant supported crown (Figure 5c).
Case Presentation
A 54-year-old adult male patient was treated in a private dental office in Padova (Italy) in January 2011. The patient was healthy, nonsmoking and with good oral hygiene. After clinical and radiographic examinations, the absence of teeth #18, #19, #30 and #31 was verified. These teeth were missed 5 years before due to periodontal disease. The use of dental implants to replace the missing teeth was planned. After local anesthesia, a total flap was performed in the left mandible, where a 10 X 4 mm dental implant with double etched surface (DAE) was placed in the area of tooth #19 so as to keep an appropriate distance from the mandibular nerve. Next, a total flap was performed in the right mandible, were a 10 X 4 mm DAE surface dental implant coated with bovine Type 1 collagen of dermal origin (custom made medical device) was placed in the area of tooth #30. Both implants were placed at crestal level and presented a 25N Torque. After implants placement, the flaps were sutured to the bone level (Silk, Ethicon 4.0, Johnson & Johnson Medical, New Brunswick, New Jersey USA). An anti-inflammatory (Nimesulide 100mg, 2 times a day for 3 days), analgesic (Paracetamol 500mg, 1 tablet every 8 hours for 3 days), and 0.12% chlorhexidine were prescribed during the post-operative, and complete oral hygiene instruction was furnished. The suture was removed after 10 days. 3, 12 months, and 6 years follow up parallel periapical radiographs were taken.
Radiographs taken immediately after surgery showed that, while the DAE surface implant was perfectly placed at the crestal bone level, distal bone around the collagen coated implant was partially missing since 4 spires were uncovered by the bone (Figure 1a and 1b). At the 1-month return, the patient was already presenting good soft tissue healing.
The 3 months follow up radiographs showed that bone around the DAE surface dental implant underwent slight preimplant crestal bone resorption since mesially, the head of the implant was no longer covered by bone and distally, the first spire of the implant was no longer covered by bone (Figure 2a). At the same follow up, radiographs of the collagen coated implant showed that bone quantity around the implant surface increased until covering the head of the implant (Figure 2b).
At the 12 months follow up, the gain in bone growth around the collagen coated implant and the bone defect around the DAE surface implant were still present with no radiographic changes (Figure 3a and 3b).
At the 6 years follow up, the radiographic bone situation was still unchanged regarding the 12 months follow up (Figure 4a and 4b). The implant supported prosthesis were still in good conditions and there was no need to replace them (Figure 5a, 5b and 5c).
Discussion
Nowadays, dental implants represent the most diffused therapy for substitution of missing teeth. Even if they are considered a safe and very predictable procedure, the literature still shows many cases of marginal bone loss around implants [16]. In the review of Al-Thobity AM et al., the authors analyzed 23 scientific articles reporting crestal bone loss around implants ranging from .05 mm to .9 mm after 12 to 96 months of follow up [17]. Even if the authors concluded that micro threaded dental implants showed less crestal bone loss, none of the studies showed a gain of bone around the implant. Moreover, in the systematic review of Al Amri MD et al., the crestal bone loss around submerged and no submerged dental implants was compared. Crestal bone loss was present in all of the analyzed studies [18].
In the case presented, a patient was missing the mandibular molars both on the left and on the right side. It was decided to replace the missing teeth with 2 different dental implants and radiographically compare them for 6 years. On the right mandible, a DAE surface dental implant coated with bovine Type 1 collagen of dermal origin (custom made medical device) was placed, and on the left mandible, the same implant with no coating was used. The radiographic results of the present study showed that the custom made medical device was stable and functional after a 6 year follow up. It was also demonstrated that around the bioactive surface of our custom made medical device, not only no crestal bone loss was present, but it was able to induce a bone gain around the implant and this gain was stable over time. On the contrary, the DAE surface implant showed slightly worst results since it was stable and functional after 6 years, but signs of crestal bone loss were present. Promising results with this bioactive surface were already obtained in an in vivo study by Cecconi et al., [19]. After placing coated and uncoated dental implants into New Zealand white rabbit femur, a 45 and 90 days comparison was made. The results of the study showed that the coated implants presented greater results in terms of bone implant contact (BIC) and trabecular thickness (Tb. Th.) when compared with the uncoated ones. The authors concluded that dental implant bone integration may be enhanced by this surface coating.
Although dental implants with traditional surfaces are still considered a great option to substitute missing teeth, this new bioactive surface may be taken into consideration for those cases in which the predictability of traditional dental implants is decreased regarding regenerated bone, low quality bone, post extractive sites and where other implants already failed.
In this case, the bioactive surface dental implant used to replace missing mandibular molars did not show any marginal bone loss after 6 years, moreover, it showed a bone gain after 3 months from its placement and kept it for 6 years while the traditional surface implant showed an immediate marginal bone loss. The use of this bioactive surface may guarantee higher success rates in the short and long terms. Additional clinical controlled randomized studies are needed to support these hypotheses.
Acknowledgements and Declaration of Interest
All of the named authors were involved in the research work and have read the paper before it was submitted for publication. All authors approved the manuscript and there is no conflict of interest to disclose.
Article Info
Article Type
Case ReportPublication history
Received: Tue 15, May 2018Accepted: Wed 23, May 2018
Published: Thu 31, May 2018
Copyright
© 2023 Francesco Saverio Ludovichetti. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.RGM.2018.10.005
Author Info
Corresponding Author
Francesco Saverio LudovichettiDepartment of Neurosciences, Department of Dentistry, University of Padova, Via Giustiniani, 1, 35131 Padova, Italy
Figures & Tables
References
1. Dieter Busenlechner, Rudolf Fürhauser, Robert Haas, Georg Watzek, Georg Mailath, et al. (2014) Long-Term Implant Success at the Academy for Oral Implantology: 8-Year Follow-Up and Risk Factor Analysis. J Periodontal Implant Sci 44: 102-108. [Crossref]
2. Mangano FG, Pires JT, Shibli JA, Mijiritsky E, Iezzi G, et al. (2017) Early Bone Response to Dual Acid-Etched and Machined Dental Implants Placed in the Posterior Maxilla: A Histologic and Histomorphometric Human Study. Implant Dent 26: 24-29. [Crossref]
3. Schliephake H, Aref A, Scharnweber D, Bierbaum S, Sewing A (2009) Effect of modifications of dual acid-etched implant surfaces on peri-implant bone formation. Part I: organic coatings. Clin Oral Implants Res 20: 31-37. [Crossref]
4. Ludovichetti FS, de Oliveira GJ, Cirelli JA (2017) Treatment of grade III furcation lesion by tunneling in a smoker pa tient: Clinical Case Report. Sci Invest Dent 22: 2-6.
5. Palma-Carrio C, Maestre-Ferrín L, Penarrocha-Oltra D, Penarrocha-Diago MA, Penarrocha-Diago M (2011) Risk factors associated with early failure of dental implants: a literature review. Med Oral Patol Oral Cir Bucal 16: 514-517. [Crossref]
6. Chiapasco M, Zaniboni M, Boisco M (2006) Augmentation procedures for the rehabilitation of deficient edentulous ridges with oral implants. Clin Oral Implants Res 17: 136-159. [Crossref]
7. Pommer B, Hof M, Fadler A, Gahleitner A, Watzek G, et al. (2014) Primary implant stability in the atrophic sinus floor of human cadaver maxillae: impact of residual ridge height, bone density, and implant diameter. Clin Oral Implants Res 25: 109-113. [Crossref]
8. de Jonge LT, Leeuwenburgh SC, Wolke JG, Jansen JA (2008) Organic-inorganic surface modifications for titanium implant surfaces. Pharm Res 25: 2357-2369. [Crossref]
9. Morra M (2006) Biochemical Modification of titanium surfaces: peptides and ECM proteins. Europ Cells and Mat 12: 1-15. [Crossref]
10. Morra M, Cassinelli C, Cascardo G, Mazzucco L, Borzini P, et al. (2006) Collagen I-coated titanium surfaces: mesenchymal cell adhesion and in vivo evaluation in trabecular bone implants. J Biomed Mater Res A 78: 449-58. [Crossref]
11. Morra M, Cassinelli C, Meda L, Fini M, Giavaresi G, et al. (2005) Surface analysis and effects on interfacial bone microhardness of collagen-coated titanium implants: a rabbit model. Int J Oral Maxillofac Implants 20: 23-30. [Crossref]
12. Baslé MF, Lesourd M, Grizon F, Pascaretti C, Chappard D (1998) Type I collagen in xenogenic bone material regulates attachment and spreading of osteoblasts over the beta1 integrin subunit. Orthopade 27: 136-142. [Crossref]
13. Dec, Gungormus M (2004) The effect on osteogenesis of type I collagen applied to experimental bone defects. Dent Traumatol 20: 334-337. [Crossref]
14. Regazzoni C, Winterhalter KH, Rohrer L (2001) Type I collagen induces expression of bone morphogenetic protein receptor type II. Biochem Biophys Res Commun 283: 316-322.
15. Mizuno M, Fujisawa R, Kuboki Y (2000) Type I collagen-induced osteoblastic differentiation of bone-marrow cells mediated by collagen-alpha2beta1 integrin interaction. J Cell Physiol 184: 207-213. [Crossref]
16. Pessoa RS, Sousa RM, Pereira LM, Neves FD, Bezerra FJ, et al. (2017) Bone Remodeling Around Implants with External Hexagon and Morse-Taper Connections: A Randomized, Controlled, Split-Mouth, Clinical Trial. Clin Implant Dent Relat Res 19: 97-110. [Crossref]
17. Al-Thobity AM, Kutkut A, Almas K (2017) Microthreaded Implants and Crestal Bone Loss: A Systematic Review. J Oral Implantol 43: 157-166. [Crossref]
18. Al Amri MD (2016) Crestal bone loss around submerged and nonsubmerged dental implants: A systematic review. J Prosthet Dent 115: 564-570. [Crossref]
19. Cecconi S, Mattioli-Belmonte M, Manzotti S, Orciani M, Piccioli A, et al. (2014) Bone-derived titanium coating improves in vivo implant osseointegration in an experimental animal model. J Biomed Mater Res B Appl Biomater 102: 303-310. [Crossref]